PMC/PubMed Indexed Articles


Indexed In
- Open J Gate
- Genamics JournalSeek
- JournalTOCs
- Ulrich's Periodicals Directory
- RefSeek
- Hamdard University
- EBSCO A-Z
- OCLC- WorldCat
- Proquest Summons
- Publons
- Geneva Foundation for Medical Education and Research
- Euro Pub
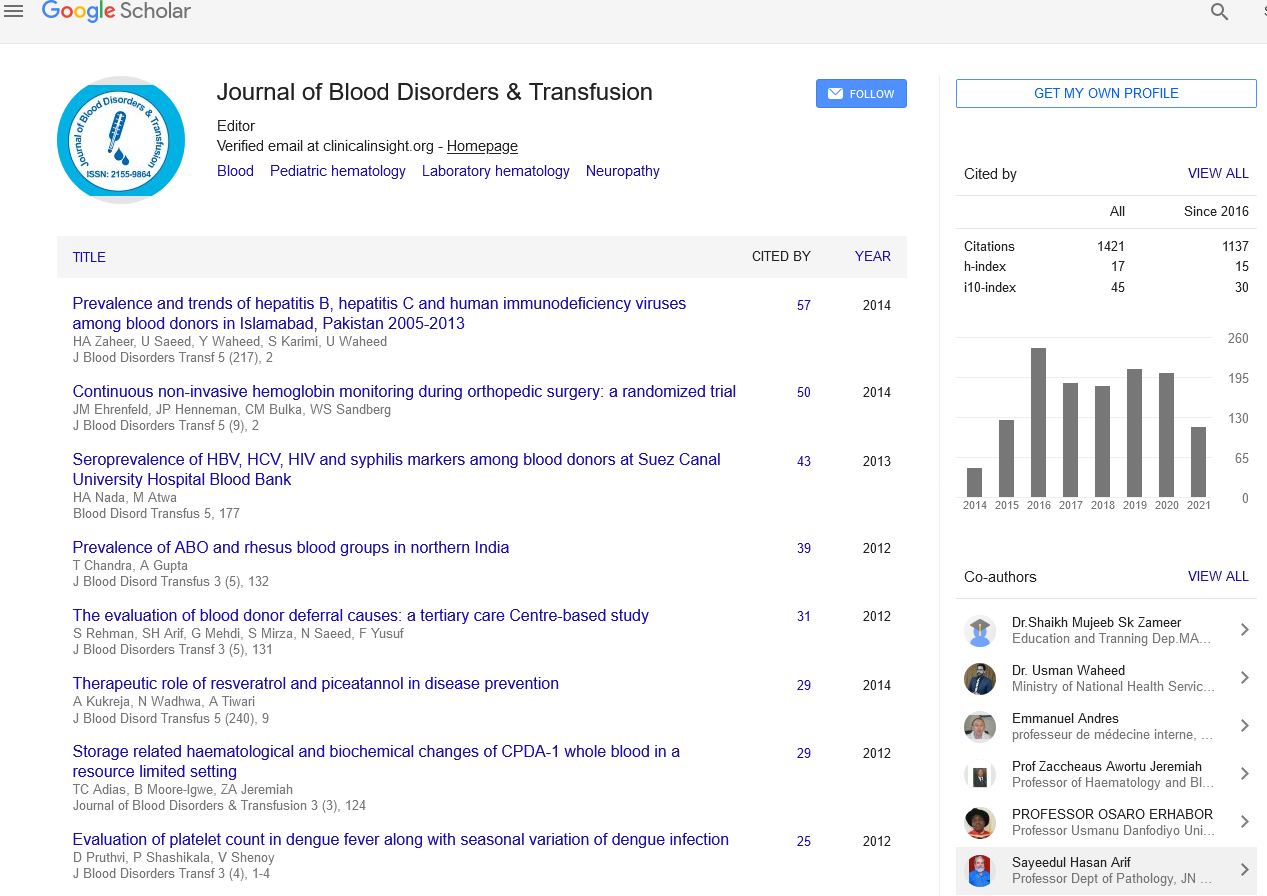
- Google Scholar
Useful Links
Share This Page
Journal Flyer

Open Access Journals
- Agri and Aquaculture
- Biochemistry
- Bioinformatics & Systems Biology
- Business & Management
- Chemistry
- Clinical Sciences
- Engineering
- Food & Nutrition
- General Science
- Genetics & Molecular Biology
- Immunology & Microbiology
- Medical Sciences
- Neuroscience & Psychology
- Nursing & Health Care
- Pharmaceutical Sciences
Cutaneous T cell lymphoma: A simulator of benign disease that requires clinical pathologic correlation to distinguish aggressive from indolent disease
2nd International Conference on Hematology & Blood Disorders
September 29-October 01, 2014 DoubleTree by Hilton Baltimore-BWI Airport, USA
Jacqueline M Junkins-Hopkins
Scientific Tracks Abstracts: J Blood Disorders Transf
Abstract:
Cutaneous T cell lymphoma (CTCL) is a primary cutaneous lymphoma that presents in all age-groups. The most common is mycosis fungoides (MF), which presents as erythematous atrophic or mildly scaly patches on double covered sites that progress slowly to plaques/tumors. The disease is indolent, and patients survive for years with a variety of topical and systemic agents. Histologically, there is an atypical lymphocytic infiltrate that is prominent in the epidermis (epidermotropism), or hair follicles. The latter is seen in folliculotropic MF, which has a worse prognosis than classic MF. Other MF variants include pagetoid reticulosis (acral; indolent course; marked epidermotropism) and granulomatous slack skin (intertriginous site; elastic tissue loss; granulomatous inflammation). The MF is typically CD3+/CD4+. Some variants (pagetoid reticulosis and hypopigmented MF) are CD8+. Variants of non-MF CTCL include subcutaneous T cell lymphoma [SPTCL], which is a fat-tropic cytotoxic CTCL CD3+/CD8+/TIA1+/alpha/beta+), gamma delta lymphoma (more aggressive that SPTCL, with a gamma/delta cytotoxic phenotype, CTCL with erythroderma and peripheral blood involvement (Sezary syndrome), aggressive epidermotropic cytotoxic CD8+ lymphoma; in contrast to pagetoid reticulosis, it involves unusual sites such as genitalia and mucous membranes, and CTCL presenting as a tumor or plaque that presents without the MF-like patch stage--CD4+ small/ medium pleomorphic CTCL and anaplastic large cell lymphoma (CD30+, ALK negative). Self-resolving papules with histology can simulate CTCL (lymphomatoid papulosis/LyP). It is imperative that the clinical presentation of the biopsied lesion be correlated with the histopathology to differentiate indolent from aggressive disease, and to exclude the self-resolving lesions of LyP.
Biography :
Jacqueline M Junkins-Hopkins, MD, completed Medical School at Johns Hopkins in Baltimore, followed by Residency in internal medicine at Johns Hopkins, residency in Dermatology at University of Virginia in Charlottesville, VA, and Dermatopathology at Harvard Medical School. She was Faculty at the University of Pennsylvania as a Dermatopathologist and Dermatologist from 1997-2008, with a special interest in Cutaneous Lymphoma. She was the Director of Dermatopathology at Johns Hopkins until 2011, and is currently a Consultant Dermatopathologist and Cutaneous lymphoma expert at the Ackerman Academy of Dermatopathology. She has published over 70 papers, with a focus on cutaneous lymphoma.