Neoplastic Limp or Irritable Hip?
Received: 26-Feb-2018 / Accepted Date: 03-Mar-2018 / Published Date: 07-Mar-2018 DOI: 10.4172/2472-016X.1000123
Abstract
A child who has an acutely irritable hip with septic picture can pose a diagnostic challenge. Although neuroblastomas are rare in children, symptoms may substantially overlap in the acute setting makes differentiation difficult. In this case report we have outlined the importance of clinical and radiological findings in two cases presented with extraabdominal neuroblastoma and the pitfalls in making the correct diagnosis. The purpose of this pictorial report is to increase awareness of orthopaedic surgeons of the possible presentation of this common childhood malignancy and deliver early prompt diagnosis.
Introduction
Irritable hip is the most common cause of hip pain in children and the clinical priority for clinicians is the timely identification and management of septic arthritis [1]. However other rare conditions such as malignancy must be considered as the differential diagnosis [1-4]. Neuroblastoma accounts for 7- 10% of childhood malignancies and is one of the most common extracranial solid tumours occurring in paediatric population [1]. It arises from sympathetic neural tissue, and therefore can occur anywhere within the sympathetic nervous system [2]. It most frequently originates within the abdominal cavity (65%) or follows the distribution of the sympathetic ganglia along paraspinal areas from the neck to the pelvis [3]. The majority (80%) of cases present in children younger than 5 years [4].
It has been well recognized that neuroblastoma conveys a widely varying clinical picture which is inherently a major cause of delayed recognition [5-7]. The most common clinical presentation of this malignant neoplasm is abdominal mass [4]. Nevertheless, 15% of cases present with hip pain or limping [5]. A child who has an acutely irritable hip with septic picture can pose a diagnostic challenge [5,6]. Although neuroblastomas are rare in children, symptoms may substantially overlap in the acute setting makes differentiation difficult and can therefore be easily missed by the admitting doctor [5].
In this case report, we have outlined the importance of neurological examination, radiological investigation and haematological factors in two cases presented with extra- abdominal neuroblastoma and the pitfalls in making the correct diagnosis. The main purpose of this pictorial report is to increase awareness of orthopaedic surgeons of the possible presentation of this uncommon childhood malignancy and deliver early prompt diagnosis by which can influence the prognosis favorably.
Case Presentation
Case 1
A 14 months old male toddler presented with 5- day history of fever, diarrhea, and difficulty in weight bearing. There was no history of preceding trauma. Child had normal developmental milestone with no significant family history. However, he had a previous hospital admission due to presenting symptoms of limping and borderline fever, almost two months earlier. He was discharged after 48 hours with an impression of transient synovitis and was asymptomatic for 7 weeks.
In recent admission, he was more symptomatic; pale, dehydrated, lethargic and anorexic. Lung and heart examination revealed no abnormality. There was no evidence of abdominal mass or organomegaly. The affected hip was held in 40 degrees of flexion and 10 degrees of external rotation. Overlying skin and soft tissue integrity were normal. Any passive movement of the affected hip induced severe discomfort. He was initially commenced on an intravenous antibiotic considering septic arthritis of left hip as the main impression. Plain radiographs (Figure 1a) and ultrasonographic studies of hip excluded any feature of osseous abnormality, joint effusion or periosteal reaction. Furthermore, neurological assessment revealed an abnormal ankle clonus in keeping with upper motor neuron lesion. Subsequently, an urgent MRI of whole spine (Figures 1b) was performed and demonstrated an extensive thoracic neuroblastoma with encroachment to the spinal canal compressing the cord between T3 to T8 levels. Furthermore, multiple extra- axial lesions suggestive of metastasis were found in right posterior occipital skull, liver and right lung. Patient was immediately transferred to paediatric oncology unit for further investigation and treatment.
Figure 1a: Pelvis radiographs [case 1]; normal bone and joint outline.
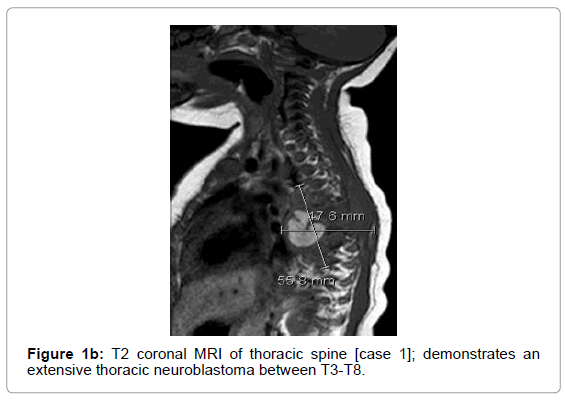
Figure 1b: T2 coronal MRI of thoracic spine [case 1]; demonstrates an extensive thoracic neuroblastoma between T3-T8.
Case 2
An eight year old boy presented with 2- day history of atraumatic left hip pain, limping and a low- grade fever. His past medical history was insignificant. His ability to weight bear was impeded by groin pain. There was no history of previous surgery, and any constitutional or prodromal symptoms. On clinical examination, the left hip was warm to touch and tender with mildly restricted movement mainly at flexion beyond 60 degrees. In addition, an altered sensation at L1 and L2 dermatomes of left thigh was identified. Laboratory tests revealed a normal WCC (6.8 × 109 cells/L) and a mildly raised C- Reactive Protein of 33 mg/L (normal 0-10 mg/L) on the first day of admission. Further plain radiographs of left hip and knee (Figure 2a) and ultrasonographic studies of abdomen did not show any specific atypical features. CRP trend was checked on day 3 and was raised to 88 mg/L. His haemoglobin was reported within a normal range (121 g/L). He became febrile again on day 4 of admission and reluctant to mobilise. Further assessment excluded any source of infection. An MRI of lumbar spine and pelvis was performed on day 6 and revealed a neurogenic solid tumour in consistent with neuroblastoma (Figure 2b). Moreover, staging Computed Tomography scan did not manifest any feature of metastasis. Cyclic chemotherapy was started as first line treatment. A 3 month follow-up MRI demonstrated a reduced volume of the tumour which is suggestive of responding to treatment. He is currently able to mobilise independently without any discomfort at his left hip (Figure 3).
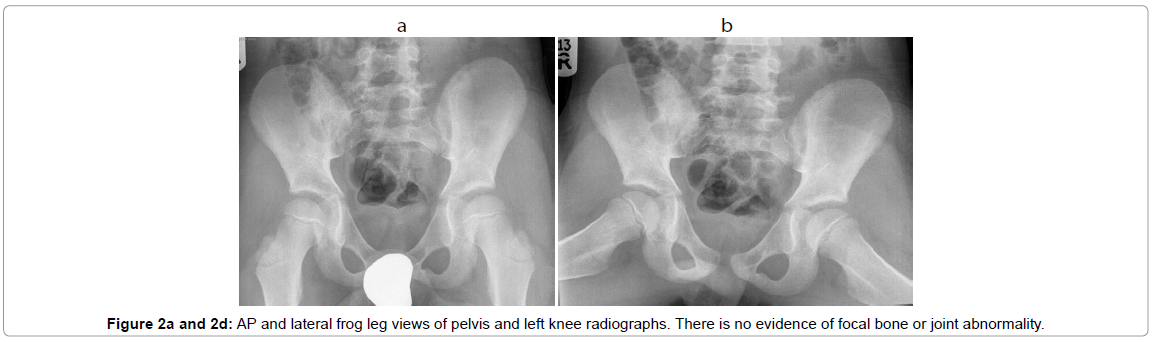
Figure 2a and 2b: AP and lateral frog leg views of pelvis and left knee radiographs. There is no evidence of focal bone or joint abnormality.
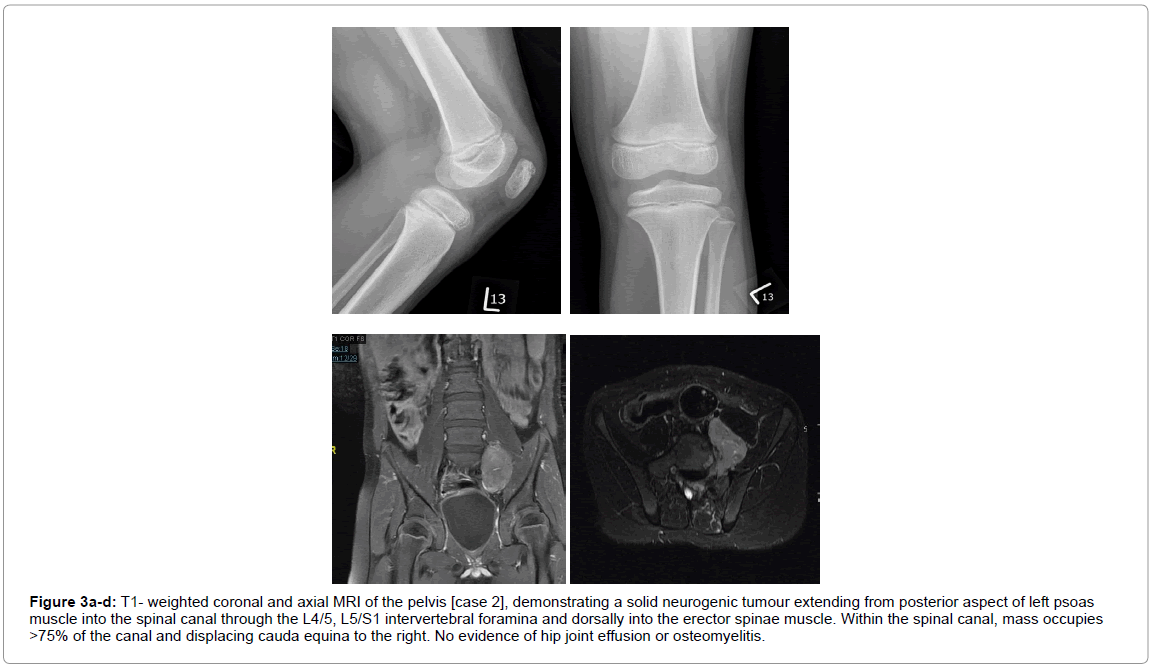
Figure 3a-d: T1- weighted coronal and axial MRI of the pelvis [case 2], demonstrating a solid neurogenic tumour extending from posterior aspect of left psoas muscle into the spinal canal through the L4/5, L5/S1 intervertebral foramina and dorsally into the erector spinae muscle. Within the spinal canal, mass occupies >75% of the canal and displacing cauda equina to the right. No evidence of hip joint effusion or osteomyelitis.
Discussion
Neuroblastoma demonstrates a wide spectrum of clinical symptoms which depends on the site, extent and the biological features of the primary lesion. Musculoskeletal symptoms such as limping, hip pain or irritable hip may dominate the clinical picture of neuroblastoma, and therefore can be easily overlooked by the admitting orthopaedic surgeon. Transient synovitis or septic arthritis is the most frequent provisional diagnosis at the time of presentation in most series [8,9]. The mean time between disease onset and the definite diagnosis of neuroblastoma has been reported to be 3.2 months [8].
Delay in diagnosis has been reported with catastrophic results and poor prognosis [6]. Metastatic neuroblastoma is evident at initial clinical presentation in approximately 60% to 75% of these cases [6,8].
Due to the nature of the cancer, therapies can include chemotherapy, surgery, myeloablative radiation, and stem-cell transplants [10]. Around a fifth of neuroblastoma cases, however, will be refractory to initial treatment [10]. Prognosis correlates with age and the degree of differentiation, and thus, outcomes vary from high rates of survival to recurrence and mortality [10].
Mohan et al. reported a case of neuroblastoma that was initially thought to be an irritable hip. They had highlighted the importance of MRI as primary imaging modality of choice for evaluation of an acute limping child. A delayed diagnosis rendered a challenging outcome with poor prognosis [5].
More recently, Parmer et al. reported four cases of malignant neuroblastoma, all presented with hip pain and were initially managed as a case of transient synovitis or septic arthritis of hip. A routine abdominal ultrasonographic study as a primary adjunct to exclude the presence of intra-abdominal solid lesion was highly recommended [7].
On the other hand, others have concluded that MRI is more informative and sensitive to delineate any abnormal signal suggestive of neuroblastoma compared to the other modalities including ultrasonography [5,11].
Learning Points
The clinical features of a child with neuroblastoma can be similar to transient synovitis, septic arthritis or osteomyelitis. Laboratory values are quite nonspecific and are not always helpful in differentiating between the entities. Neuroblastoma should be considered as one of the main differential diagnoses in all children presenting with hip pain, limp and or an abnormal neurological test.
• Neuroblastoma can present as an irritable hip
• The history and clinical examination are often misleading and children are unable to verbalise their feelings.
• A high index of suspicion, appropriate clinical examination (particularly neurological assessment) and early investigation are integral in the diagnosis and help distinguish between inflammatory and neoplastic aetiology.
• Close monitoring for first 3 months is strongly recommended if patient is due to be discharged within 24-48 hours.
• MRI should be considered as the preferred modality of investigation in suspecting cases to avoid further delay in diagnosis.
References
- Dormans JP, Moroz L (2007) Infection and tumors of the spine in children. JBJS (Am) 89: 79- 97.
- Kushner BH, Cheung NKV (2005) Neuroblastome - from Genetic Profile to Clinical Challenge. N Engl J Med 353: 2215-2217.
- Maris JM, Hogarty MD, Bagatell R, Cohn SL (2007) Neuroblastoma. The Lancet 369: 2106- 2120.
- De Bernardi B, Balwierz W, Bejent J, Cohn SL, Iehara T, et al. (2005) Epidural compression in neuroblastoma: diagnostic and therapeutic aspects. Cancer Letters 228: 283- 299.
- Mohan A, Gossain SR (2006) Neuroblastoma: A differential diagnosis of  irritable hip 72: 651-652.
- Wong M, Chung CH, Ngai WK (2002) Hip pain and childhood malignancy. Hong Kong Med J 8: 461-463.
- Parmar R, Wadia F, Yassa R, Zenios M (2013) Neuroblastoma: a rare cause of a limping child. How to avoid a delayed diagnosis? J Pediatr Ortho 33: 45-51.
- Trapani S, Grisolia F, Simonini G, Calabri GB, Falcini F (2000) Incidence of occult cancer in children presenting with musculoskeletal symptoms: a 10- year survey in a pediatric rheumatology unit. Semin Arthritis Rheum 29: 348-359.
- Aston JW (1990) Jr., The orthopaedic presentation of neuroblastoma. Orthop Rev 19: 929-932.
- White PM, Boyd J, Beattie TF (2001) Magnetic resonance imaging as the primary imaging modality in children presenting with acute non traumatic hip pain. Emerg Med J 18: 25-29.
Citation: Amin K, Randeep A, Urjit C, Radhakant P (2018) Neoplastic Limp or Irritable Hip? J Orthop Oncol 4: 123. DOI: 10.4172/2472-016X.1000123
Copyright: © 2018 Amin K, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Select your language of interest to view the total content in your interested language
Share This Article
Recommended Journals
Open Access Journals
Article Tools
Article Usage
- Total views: 6704
- [From(publication date): 0-2018 - Dec 19, 2025]
- Breakdown by view type
- HTML page views: 5694
- PDF downloads: 1010