A Qualitative Study of the Experience of Miscarriage from Patients and Providers in the Rural U.S.
Received: 01-Nov-2018 / Accepted Date: 28-Jan-2019 / Published Date: 04-Feb-2019 DOI: 10.4172/2471-9846.1000224
Abstract
This qualitative study examines how female patients in rural communities in the Midwest, who experienced at least one miscarriage, perceived their experience of pregnancy loss. Qualitative data were collected from 10 women who did experience at least one loss in addition to 10 participants who were providers or partners of the women were interviewed. The Socio-Ecological model informed the methodology and thematic analysis. Open-ended qualitative interviews provided the basis for the analysis. Transcribed narrative data were analyzed using standard coding procedures and MAXQDA software. Women who experienced miscarriage discussed how they made meaning of the experience within the context of care and their perceptions of risk given certain socio-environmental factors. Providers, public health professionals and family studies professionals can use the study results to better inform best practices in maternity care particularly in under-served, resource-poor locations.
Keywords: Miscarriage; Gender; Public health; Patient perspectives; Risk; Qualitative analysis; Reproductive uncertainty; Women’s health; Provider perspectives; Case study; Socio-ecological model; United States
Introduction
Approximately one in four of all pregnancies end in miscarriage [1-3]. In the United States, miscarriage is the most common reason for gynecological admissions into hospitals and yet research over the past several decades indicates [4,5] that the experience of miscarriage is both ubiquitous and under-recognized by patients, providers and the public writ large, and across many cultural contexts. Miscarriage and the perceptions of risks associated with it, is an experience, which while common, goes largely un-discussed in contemporary culture or public health discourse and is rarely seen as a significant public health problem. Over the past century, and with heightened attention to both reproductive health care and assisted reproductive technologies and against a backdrop of increasing age of childbearing (for both men and women), researchers have discovered particular risk factors for miscarriage. Commonly cited risk factors include the age of the mother: miscarriage risk rises as maternal age increases. For women under 35 the clinical miscarriage rate is 6.4%, at 35-40 it is 14.7%, and over 40 it is 23.1% [6]. Cigarette smoking, certain drugs (prescribed drugs such as aspirin or illicit substances), multiple pregnancies such as twins or triplets, poorly controlled conditions such as diabetes, and auto-immune disorders such as Lupus may also increase the risk of miscarriage. More recent studies focus on caffeine intake, exercise, weight, the presence of particular kinds of antibodies in the bloodstream, thyroid concerns and socio-environmental factors as significant contributors to potential miscarriage.
But if miscarriage is the most common adverse outcome in early pregnancy, it unfortunately remains one of the least understood and discussed phenomena. For many women, it is a traumatic experience and one with little broader social and cultural support or recognition. Research has identified shortcomings in the emotional and social support provided for miscarriage sufferers but, personal accounts, and in particular the perceptions of risk that led to the experience of pregnancy loss remain relatively under-explored [7]. Studies suggest that anxiety and emotion support among couples can aid greatly in the treatment of grief, isolation and even of the understanding the health problem, but do little to ameliorate the individual perceptions of risk or management of identity that individuals experience as a result of miscarriage [7]. By understanding the significance of individual perceptions of risk and provider, partner and patient roles in pregnancy loss, we might ascertain what it means to navigate the experience of miscarriage.
Literature
While miscarriage is an ubiquitous experience, the systematic study of miscarriage, perceptions of and management of it has been relatively understudied [8]. The majority of studies have tended to focus on causal factors and links, and several psycho-social studies exist that examine the experience of grief, impact upon family dynamics and relationships, and mental health after miscarriage [9-11]. Despite these scholars however, a good deal of the research remains focused on the meaning of miscarriage as related to the physiological ability to carry subsequent pregnancies to term rather than emotional or socially constructed responses, which as those authors suggest, is a much-needed approach to the study of pregnancy loss. Some studies, albeit few, focus upon male factors influencing miscarriage outcomes and few, if any, interrogate questions of male perceptions and experiences of pregnancy loss [12]. Yet little data exist to situate miscarriage in contemporary discourse about assisted reproductive technologies, the implications of miscarriage, on both patients as well as providers, and how perceptions of and the management of miscarriage occurs in resource-poor areas (and under-served areas such as those in the rural Midwest) of the United States where ob/gyn services are limited and this research seeks in part to help fill that gap.
Risk and miscarriage
True rates of miscarriage are difficult to discern [5]. As a result of the relative invisibility of miscarriage and methodological challenges of capturing real “rates” in the population, it was far more useful to discuss how the concept of “risk” plays an important role in perceptions of miscarriage in this particular study. In this study, participants were asked to think about their understandings of risk and factors that would or could contribute to the cause of miscarriage. These perceptions of risk and responses to the experience of miscarriage were understood as qualitative data that reflected a patient’s perspective. An ecological system theory is useful in understanding these data. For example, while the woman who experiences a miscarriage is often seen as the primary or only individual involved, it is necessary for providers and public health practitioners to recognize the myriad support systems, the social network in which an individual is immersed and to identify the factors in any socio-ecological environment that some individual sees as a significant factor in the experience of miscarriage.
Miscarriage as a public health problem
Reproductive “disruptions” such as infertility, pregnancy loss and fetal genetic disabilities can be tremendously anxiety-producing for those who experience such events. Scholars have situated recent discourse on reproduction in debates over what may be considered “normal” reproduction given advances in technology and assisted reproduction, as well as what the global, political and policy implications of those debates may be [13]. Despite a long social history and feminist scholarship on the phenomenon of miscarriage, pregnancy loss remains largely a medicalized issue for those in health care and sciences.
In the United States, the phenomenon of miscarriage and pregnancy was long documented in women’s lives and yet is rarely discussed in medical texts or manuals [14]. Up until the 1960s and 1970s in this context, miscarriage and pregnancy loss remain shrouded and relatively unexamined as a public health problem-remaining solely an individual concern and an issue for an individual patient and their provider in minimal ways. More recently however, public health awareness movements [15] and greater attention to pregnancy loss as part and parcel of reproductive health [16-18] have meant that women have been encouraged to acknowledge grief over pregnancy loss and that that acknowledgement and attention has occurred beyond the boundaries of women’s health magazines and into hospital settings.
Awareness of miscarriage has come about in public health in part as a result of discourse over abortion, feminism and medical control over reproductive bodies. It is also clear that an uncritical adoption of definitions and language used to describe miscarriage by hospitals, health professionals and therapists have contributed in part to the arguably still shrouded, stigmatized and complex problem of pregnancy loss.
Socio-cultural, individual and environmental factors-using an ecological framework
The majority of Americans inaccurately believe miscarriage is rare and misunderstand its causes, creating an often isolating and guiltridden experience for those who experience it. These are the findings in the first-ever national survey in 2013 from the Albert Einstein College of Medicine to assess attitudes and perceptions towards miscarriage. Over one thousand participants (both women and men) believed miscarriage is rare (about 65%), when as noted previously, it occurs in one in four pregnancies. This study reinforces the statistic that the majority of miscarriages (60-80%) are due to chromosomal abnormalities; however, survey respondents most commonly cited a stressful event (76%), longstanding stress (74%) and lifting a heavy object (64%) as causes. Additionally, respondents inaccurately thought that having the following would cause miscarriage: a sexually transmitted disease (41%), an abortion (31%) or use of implanted long-term birth control (28%). In this study, nearly 23% of respondents erroneously believed a miscarriage may be caused solely by the woman not wanting the pregnancy or feeling ambivalent toward the outcome.
While knowledge of miscarriage rates was low, respondents in the 2013 study accurately assessed that it is traumatic, with 66% believing the emotional impact is severe and potentially equivalent to the loss of a child; the language used to describe both miscarriage and stillbirth are captured in medical literature as “pregnancy loss” and arguably create perceptions and attitudes toward treatment, social responses and care that stigmatize and shroud miscarriage in clinical (rather than patient driven) terms; ultimately hindering effective communication or treatment of miscarriage and risks as public health problems. Research shows understanding the cause of miscarriage can reduce feelings of guilt or blame [6,19,20]. Interestingly, public disclosure of a miscarriage by a celebrity or public figure had a positive influence on the feelings of those who had suffered miscarriages. The study noted that “false perceptions and lack of understanding about miscarriage are significant in the U.S., and contribute too many women and couples feeling isolated and alone after suffering from a miscarriage… widespread education is needed to reduce stigma and help those who have suffered an early pregnancy loss. Patients should work closely with their doctors to understand the causes of their miscarriages and to work towards successful future pregnancies.” Yet provider perspectives arguably remain limited to a medical model of the body [21] and may overlook significant sociocultural, demographic factors. This may be particularly true in the case in rural, resource-poor communities, both in the U.S. and in any work abroad. Increasingly too, with later age of childbearing among women in the United States, age related complications and factors related to pregnancy loss have taken center stage in discourse surrounding miscarriage and assisted reproduction. According to the Albert Einstein College of medicine study, “sub-fertile” women who are using assisted reproductive technologies experience greater psychological trauma after miscarriage than others, they expect to be able to achieve fertility with more reliability given the utilization of technology. Reliance on assisted reproductive technologies and presumptions about access (not all socio-economic and demographics will have equal access to costly interventions/technologies), on the part of both patients and providers can hinder investigation into miscarriage itself as a significant and socially relevant public health problem. Participants in this research study as well, reflected similar assumptions and support the use of the socio-environmental explanatory framework. Specifically, it was important to examine the beliefs and interactions between individuals at multiple levels of interaction [22] in order to help explain responses by patients as well as providers. An ecological system theory assumes that humans are social, and interaction between individuals can be the best lens through which to examine behavior and belief systems (Figure 1). Ultimately, the ecological framework takes into account the cultural context, interpersonal relationships, socio-economic status and networks of support and information flow that help to define and perhaps determine perceptions of risk and the management of miscarriage by individuals.
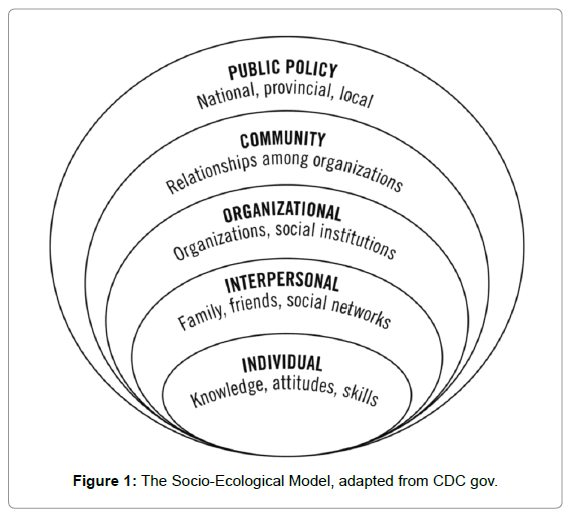
Figure 1: The Socio-Ecological Model, adapted from CDC gov.
Provider perspectives on miscarriage
As noted previously, approximately15% of recognized pregnancies end in miscarriage, or spontaneous abortion; the proportion increases with the sensitivity of pregnancy diagnosis to a range of 20%-62%. Using a conservative incidence estimate of 10%, there may be half a million spontaneous abortions each year in the United States. Quality health-care for miscarriage typically means that women are seen in physician’s offices, uterine aspiration is typically conducted and in particular cases, emergency room visits are necessary if resources are available and patients need to be (or should be) seen after miscarriage (for D & C procedures or general follow up). Surgical management, in the case of early pregnancy failure is often the norm for those who have access and resources and little discussion between patient and provider is considered necessary [23,24] miscarriage follow up (D & C procedures primarily) are seen as standard treatments and follow up. For those in this study, not all sought or were able to seek clinical care immediately after miscarriage, but were aware of services through the hospital or alternative care centers. There are significant studies regarding the question of compliance in reproductive health, and specifically when talking about the meaning of miscarriage. For many providers, women’s willingness and ability to comply with provider recommendations, care, and “well-pregnancy” goals become contested and the source of frustration for many - prompting a “why don’t they just do what I say?” kind of response in some of the interviews and in discussion of risks for miscarriage. For women in rural and resourcepoor areas, the ability to adhere or comply with particular guidelines suggested by physicians or “well-baby” initiatives to reduce the risks of pregnancy are not part of cultural perceptions of health. For example, several studies note the role that cultural context and the influence of culture can play on women’s decision making while pregnant, and these studies mirror much of what individuals in this study discussed when talking about patient versus provider care for reproductive health and pregnancy loss [25]. Largely absent from discussions of knowledge and awareness of miscarriage is any mention of the role of men and/ or systematic study of perceptions or responsibility in compliance or complicity in adherence to drug regimens prescribed for pregnancy. Much of what the provider perspective rests on is the desire of providers to see patients adhere to particular “healthy” pre-natal strategies [5].
Public health responses to miscarriage
An emphasis on grief and grieving may easily be seen as apolitical [14] - certainly grief and an increase in awareness of the necessity for sensitivity to grief and pregnancy loss has been put into place as a means to ameliorate structural and societal inattention to the meaning and management of miscarriage. Nevertheless, attention to and public health responses to miscarriage can have certain politicized implications. For example, “public fixation on miscarriage as a personal tragedy rather than a public-health problem is certainly politically advantageous for American pharmaceutical, chemical, manufacturing, and agricultural industries, that might otherwise face restrictions” [14]; if the onus and responsibility for the pregnancy loss is at the individual and behavioral level, than other structural, community and policy level factors need not be explored or addressed. If environmental factors contribute directly to increases in miscarriage incidence [26-28] they may have larger implications beyond individual health concerns.
Additional important literature on the role of caregiving for those who experience miscarriage indicates the positive outcomes from counseling and recognition of the experience beyond the individual [9]. Here, the data demonstrate that women’s well-being is greatly enhanced in the long-term by the recognition of miscarriage as a significant health event and the role that support and effective treatment can play in positive long-term outcomes. The insistence on viewing miscarriage as an individual health problem (rather than a public health one) also deflects attention away from inequities in health care, socio-economic and racial and ethnic disparities that produce higher infant mortality rates among some populations, such as among African-Americans in the United States or among cultural groups in cross cultural contexts [14,20,29]. Lastly, as medical institutions legitimate and support individual responses and factors as the sole contributors to miscarriage and pregnancy loss, it serves to reinforce anti-abortion, anti-feminist perspectives that suggest ideological stereotypes of woman as mothers, conventional gender norms of gender and family, the primacy of motherhood in defining women as persons and ultimately, the need for less attention by those working in public health to address miscarriage as a serious issue. The assumptions that undergird these perspectives are that women grieve and are sad at pregnancy loss and that is the sole, expected or appropriate reaction - obviously this will vary by life cycle stage, and other socio-cultural factors, but those are secondary factors, and miscarriage remains cast as an individual problem and not necessarily a public health one [14].
Methods
Participants and context
Ten women who self-identified as having experienced at least one miscarriage were recruited for this study. Additionally, five partners of the participants and five providers were included. To be eligible for participation, individuals were over the age of 18, reported having had (at least) one miscarriage in the past 5 years (for women and their partners) or having treated a patient who miscarried during that same time frame. The rationale for these inclusion criteria was that individuals who experienced miscarriage may forget certain detail some of their responses and reactions to the experience over time. Snowball sampling was also used within the group. Participants were asked to recommend other potential participants who shared their socio-economic, geographic location and experience of miscarriage and allowed a focus on particular cases in great depth [30]. The snowball sampling method was particularly useful given the relative invisibility and potential sensitivity of miscarriage in everyday life, requiring additional knowledge and levels of familiarity and rapport between participants and the researcher.
This study was conducted in the rural and under-served communities in Putnam and Hendricks counties in central Indiana. These two counties were initially selected for their ease of accessibility to the researcher and an attempt to reflect some diversity in study population. Putnam County is significantly less wealthy as a county than Hendricks County with one hospital serving approximately 38,000 people throughout the 483-square mile region. The majority of individuals live in rural areas and contrasts are sharply divided between those who are farmers and those who work for larger corporate distribution centers. Greencastle is the county seat where the largest employer is a residential liberal arts university and is the site of the Putnam county hospital and clinical ob/gyn resources. Unemployment in 2010 for Putnam county was 6.5% and the county is 97.3% white, 4.1% identify as African-American and the remainder Latino or mixed ethnicity according to the U.S. Census in that year. Hendricks county, by contrast, had a larger population of 150, 400 people in 2010, spread over 409-square miles with an unemployment rate of 4.9%. The county seat is the community of Danville which is host to a growing community of midwives and doulas, and the Hendricks county hospital system is one of the most extensive in the state (second only to the Indiana University medical system). Hendricks county also has a slightly more diverse racial/ethnic demographic (although not much) where 89.8% of the population identifies as white, 5.8% as African- American and 3.4% as Latino and the remainder consisted of two or more ethnicities. The study counties were therefore largely white, rural and poor communities and the study participants reflective of the demographic snapshot of these areas.
Recruitment
After the project received institutional review board approval, participants were recruited through electronic mailings and by posting announcements on discussion boards online and through local pregnancy loss support groups. Permissions were obtained before any postings or outreach and all participants were contacted with information about this study to determine whether they were willing and able to participate in advance of any interview. Both men and women were recruited and consented by the researcher. The primary method of data collection included interview and longitudinal participant observation with the study participants and all data were collected by the researcher. Additional and periodic informal conversations were held with study participants in order to discover common themes in the understanding and perceptions of miscarriage - and included both patient and provider perspectives.
Data Collection
Interviews: All participants took part in face to face interviews that lasted between 60-90 minutes. Informed consent was obtained prior to each interview. The interviews were conversational in style, were semistructured and included demographic information, questions of health status, health awareness and literacy, and perceptions of and responses to the experience of miscarriage. Given that the socio-ecological model drove the theoretical approach to this project, questions reflected experiences in a variety of spheres of social interaction and were particularly designed to emphasize health literacy about physiological and environmental risks as well as socio-cultural perceptions of miscarriage. Interviews were conducted with participants in order to elicit responses about the lived experience of miscarriage and the management of that experience in light of those risks and perceptions. While all individuals in the study had different specific experiences and perspectives (for example women, their partners and their physicians/ providers), the qualitative approach in this study means that patterns in the data were discernible even from the range of narratives collected [31].
Analysis: After transcribing an interview, notes were made of participants’ statements about the miscarriage experience - either their own or that which they observed as partners or health care providers. This inductive approach is utilized as part of thematic, phenomenological research [32,33] and illuminates common themes in coded data. Transcripts were reviewed multiple times and relevant themes, those that appeared in multiple transcripts, were recorded. The interviews, case study narratives, and participant observations were not anonymous, but all coded notes have been cleaned of any confidential or identifying information so that no data can be linked in those ways. All transcripts of interviews and follow up conversations were recorded and transcribed by the researcher with themes and codes compiled in a codebook. Coding was done by hand and with the use of MAXQDA software.
Once the relevant themes were identified they were shared with participants in order to conduct additional reliability checks. This set of checks helps to provide depth as well as breadth to the analysis [22] and reflects the iterative nature of the process. Participants also noted that investment in the research process greatly influenced commitment to the project and rapport amongst researcher and the community. After the final themes were verified by participants, a final codebook was developed. Literature related to the particular patterns in the data were sought and the data were analyzed in context of the socioecological model in public health. The ecological approach addresses the multiple determinants and levels of determinants that influence health and health behavior and helps to suggest the myriad, complex and inextricably linked behavior-related aspects of public health issues. It emphasizes multiple levels of influence and the core concept that behaviors both shape and are shaped by the social environment. Ultimately, readers of this study should be able to better understand the multifaceted and interactive effects of individual and environmental factors that determine behaviors and beliefs about the experience of miscarriage and to be able to better identify important places where policy and advocacy for better understanding of those experiences might be enhanced.
Results
Results are organized around themes related to perceptions of risk and strategies for the management of miscarriage by patients (along with their partners) and providers, and include: trust, control, blame and isolation, environmental factors, gender and an over-arching theme of the mechanization of the body.
Patient perspectives
Individual responses to questions about the meaning of miscarriage and the management of the body varied but could be organized according to certain salient themes. Specifically, narratives of patients coalesced around ideas of miscarriage as particularly gendered, clinical constructions of the body, environmental risks and public/private dichotomies.
Gender and failed identity
Perhaps the most significant theme that emerged is the idea that miscarriage and pregnancy loss are inherently gendered experiences. They are not simply reproductively different experiences for women and men, rather the social construction of the experience of miscarriage itself was understood as “naturally” and inherently different according to gender and societal expectations that surround the meaning of pregnancy and loss. The case of Karen and Steven Glazer offers insight into some of the gendered differences in responses to miscarriage.
Karen and Steven describe themselves as “active, busy people, always on the go” and as “people who find it hard to leave people behind”, even as they have moved around a considerable amount for education and employment, stressing the importance of social ties and a close network. The two married while in graduate school and as they each described it, “made the decision to finish our degrees, get good jobs together and then think about starting a family when we had more stability”. After several temporary and term positions at colleges and universities in the Midwest, the two found themselves in the fortunate position with full-time academic jobs at the same institution.
It was several years still before Karen and Steven planned to have children but as Karen put it, “we felt like we had checked off the first two steps, we had done our degrees, we had the perfect jobs together... of course we kinda felt that the next step in the plan would just fall into place”. The two decided to wait until Karen had completed her first performance review but both agreed that waiting until tenure would be “pushing it”. As Steven described, “I think we both acknowledged that we weren’t getting any younger, we felt confident but I think these days you’d also be foolish to look around and not realize that people our age who were not in academia already had kids”. Both worried too that when they had children that “the kids wouldn’t have anyone to play with in the family...my brother has children already and Karen’s brother and sister all have kids and we really didn’t want ours to be without that cousin network”, Steven relayed. Once they began trying to conceive, Karen described how “it wasn’t much planning [laughs] we didn’t really worry too much, we just thought it was pretty nice to not have to think about birth control, it felt like a relief!” and reflected on how “naïve” she felt they were then, “we didn’t even think about the possibility that something would happen that would be a barrier to conception that we hadn’t been responsible for.”
After trying to conceive for several months, it was a relief again when Karen finally became pregnant. Karen described the increasing anxiety and feelings of failure that she had begun to experience (prior to pregnancy) and reflected on the intersections between gender and reproduction:
I was getting really anxious...like sex wasn’t even as fun anymore, we were completely trying....having ex all the time it felt like...but not in the way that we used to like on vacation...[laughs]...this was beginning to feel like a job and then the hard part for me anyway was that the job was something that I was turning out not to be very good at...it was ironic because I had just gone through such a successful job review but I felt like such a failure in everything related to my body... I just felt like this is something that a woman should be able to do.
Karen’s description of the challenges in getting pregnant a first time resonated with Steven but as she correctly summarized, his interpretation of what was happening and how they were each experiencing this early frustration was less about failure as an individual and more grounded in sympathy for his partner. Steven talked about how he had his own expectations that “things would eventually work out” and described how when Karen finally became pregnant:
I think I just expected that it would work out all along, maybe that’s a guy thing, I don’t know, I’m not sure what other guys would have to say about that but I do think that the expectation for men is far different than for women. I mean nobody, nobody at all who knew we were trying ever even questioned me about what I was eating or drinking or doing and Karen got those questions all the time, she was constantly monitored even in informal ways, we used to joke about it like the prepregnancy panopticon [laughs]...we were expecting that people would monitor a pregnant Karen, like no-alcohol, no caffeine, stuff like that, but this fertility monitoring was tough! It felt like we might as well be having sex in public sometimes...I would get a call, email or text from Karen during the day if she was ovulating and we’d have to rush home or find some way to plan to have sex if not then, later in the day.
At twelve weeks into the pregnancy and at the third physician’s visit, after which Karen and Steven had planned to tell people their news, it became clear that the pregnancy was not viable. Karen described the experience this way:
The doctor was looking and looking for a heartbeat, and he was looking and looking and not finding it and it was this terrible, like, ‘I have to leave the room’….and then he came back with different equipment, the ultrasound and then there was nothing there. And the title he gave was blighted ovum, very medieval, and some of the terminology is real interesting, really kinda coarse and harsh....so...blighted ovum [pause] basically it had never developed a heart but….my body hadn’t rejected the placenta….it was attached maybe? ...the uterine wall, it was there, everything was still there and kinda operative….and I was three days from leaving for a trip with students and they had to do a D & C right away and so we scheduled the D & C for the next morning. And I remember coming home just sort of shocked and you know, the shock of it all…
Karen described feeling devastated and “like all those old feelings of failure came right back up” for her. She described feeling tension between her own internalization of failure as she stated as “literally a failed reproductive body” but also the frustration that “this wasn’t happening to Steven...it was one of the things that we couldn’t totally share, I mean he was there and sharing in it and was sobbing, but it was happening to me, to me as a woman.” For Steven the experience of that first miscarriage was profound but in ways that he reflected upon as a “learning experience”. He stated, “I really felt like it was a learning by doing kinda process and here we were totally crushed, I mean just so, so sad and it was so painful for Karen, but we learned from it and moved on, we cried alot and hurt, but yeah, it made us optimistic.”
For Katrina and Paul Roberts, who describe themselves as well-educated “but struggling to make ends meet”, the experience of miscarriages highlighted the tremendous differences in public responses to failed pregnancy in terms of gender. Specifically, the difficulty that many men experience in talking about their experience of miscarriage or even the difficulty in getting others to recognize that the miscarriage was a shared experience. For several men, it was clear that while pregnancy was seen as something that happened to the couple, miscarriage was something that was culturally understood as happening to women. Paul, in talking about their first experience stated:
The first miscarriage really hit us both hard, it was really difficult, I just couldn’t express it to anyone how hard it was hitting me, it felt like it was something that was totally taboo. People at my office were asking how Kat was and I just felt like screaming sometimes so they’d hear me too...you know? Like nobody ever, ever, ever asked me how I was doing, like its completely taboo to ask a guy about it. It was weird, like when we announced we were going to have a baby it was something that was about us, but when people found out it was a miscarriage, it was about her.
Paul noted too that his identity as a “father” was subject to scrutiny as well. Whereas his wife was “seen” as having experienced pregnancy and therefore motherhood to some extent, Paul described feeling invisible and subject to some debate over whether or not he could claim any legitimate identity as a father and observed that the same simply was not true for his wife.
Yes, it is true, not very many people go out of their way to talk to me, ask me how I’m doing, they ask about Kat but it is almost like miscarriage makes men invisible, or maybe people assume we are impervious to the pain of it, the loss is something that Kat experiences but nobody thinks that I would, I’m not going to have any Father’s Day in the future you know but nobody thinks about how this is for men, what this does to us, here I am feeling completely sad and like everyone would laugh if I suddenly whipped out the ultrasound photos we got early on or talked about my kids who died, that would not be cool.
The results from this research clearly indicate that, where pregnancy loss is approached as a gendered event, which requires reflection, explanation and the development of an appropriate ritual, there is increased opportunity for parents to articulate their own interpretation of the experience [2,34]. Yet gender remains a powerful influence on the perception of who can “claim” the miscarriage experience and how others might interpret the meaning of that experience for men and women. For example, often when a baby is stillborn, a birth certificate is required, and “serves as a ritualistic affirmation that bereavement has taken place” [2]. One man however, expressed how his grief was heightened when he tried to register his stillborn daughter only to find that, since he was not married to the mother he was unable, legally, to register the stillbirth. For many men such as Paul Roberts, social interaction and lack of more formal, legal acknowledgement of miscarriage and pregnancy loss reinforces the idea that these are inherently gendered experiences and that they cannot claim a “miscarriage” identity in the same ways as women.
Gender and age
For several individuals, the theme of miscarriage as a wholly gendered experience was also complicated by age. While Karen and Steven ultimately described at times, very different interpretations of the miscarriage, these descriptions were grounded heavily in gendered discourse about the body and age and ultimately how age matters more for women than men when thinking about reproductive ability. Their experience mirrored those of others in this study; specifically, the older the couple or individual who experienced the miscarriage, the greater the urgency and frustration expressed. For those who were younger or who had only experienced one miscarriage thus far, the responses were more positive, more optimistic. Steven elaborated several times during one of our early discussions together on how he would have been happy to wait even a bit longer to have children although he was cognizant of the fact that Karen’s fertility was at risk the longer they waited. As he described at one point:
Well for me of course, this is not something I would be doing if we weren’t together..[laughs] it’s like having the dog, I probably wouldn’t have the dog, or any dog, like I wouldn’t have thought about that as an idea if I was just a single guy, on my own and all that...[laughing] which when I think about it is ridiculous because most of my adult life I’ve been married, but I mean, I’d had my two kids in my first marriage, pretty early on and now they’re grown up...and so no, I don’t think that at this stage in my life this would be something that I’d be doing... you know you don’t see men who go to sperm banks or whatever and really want to be single fathers later in life you know, it is such a gendered thing that is for sure...and in a weird way that is a lack of power [laughs], I know that you will laugh at that and think otherwise... but you know, you know what I’m saying here, that men lose some of that power to have those choices, like if you really wanted to be a single father later in life...anytime in life maybe, you don’t have those same options, it’s completely skewed.....
As he later put it too, “men just have that luxury, we really don’t have to think about it in the same ways but we had been so focused on Karen’s job that I think it was easier to forget that the clock was ticking”. The problem raised by the miscarriage however was that the pressure was on to fulfill their fertility desires in ways that their work lives and decisions had limited.
Lastly too, the public and private performance of fertility and the challenge to gendered identity became heightened after the Glazer’s miscarriage experience. For Karen, she described a sense of relief again over the decision “not to tell” others about the pregnancy even though they had “almost made it” to the three month point. She talked about how she “didn’t want other people to then have to say something or feel sorry for me or to not talk about their own pregnancies or kids, I think that happens all the time and it would’ve just added to the sense of failure”. Interestingly for Steven, as many men who are willing to talk about the meaning and experience of miscarriage, the response was the opposite. As Steven described, there was this one time, I was in the gym, and this was right after it happened, maybe about a week or so after and this guy is in the locker room, I mean it’s a real guys guy type scene and I’m almost embarrassed to talk about it, but it was, it was so testosterone-filled...anyway, this guy from a different department is in there and he was talking smack with this other guy, they’re part of the noontime basketball crowd and that’s pretty competitive as a group...so this guy shouts at one point, and I mean he didn’t even know, nobody knew what we had just gone through, but he shouts ‘oh at least I can get my wife pregnant, knocked her up again!’...like it was a challenge or a one up…and part of the point you know, he is an older guy so it was like this double thing, double message about how virile or whatever he was...you know that’s the stuff I wouldn’t think twice about before but all of a sudden I took it personally and was thinking about what a complete asshole that guy was.
Throughout my conversations with Karen and Steven, it was clear that the meaning of their miscarriage was complicated by expectations of success in the workforce and as gendered bodies that were subject to biological realities such as age; Karen felt as though she needed to establish a career before starting a family but that control over work and family was challenged by the experience of miscarriage.
Control
Both men and women in the research talked about the “loss of control” that having a miscarriage presented in their lives. For many men, pregnancy loss signaled a profound shift in the expected future plans and direction of their lives. As she notes “when a pregnancy ends there is not only the loss of the baby, but also a loss of future hopes and dreams” [2]. Attendance a grief support groups and participation in on-line discussion and blogging groups was something that both men and women in this study did, largely, as Nicole Reitman suggested “as a result of that feeling like everything else was out of control...I felt like I’d lost everything in an instant, in that short span of time I went from being a mom to being nothing...and I had absolutely no say whatsoever, it was all out of my hands”. As Dave Forester, a self-described “working class and regular guy”, explained too.
I’ve always been a ‘take charge’ kinda guy, you know I was the first one to organize a team in the neighborhood growing up, or to do the office betting pool for March madness these days and I just have always been someone who likes to be in control [laughs] I admit it, but that was the thing when we had the next miscarriage it just felt like everything was spiraling out of control....like I suddenly had no say in anything that happened...I couldn’t stop the first one and obviously I couldn’t stop the next one...it was awful.
The lack of control over public recognition or the acknowledgement of death was also significant. Certification can serve as a ritual and symbolic affirmation that pregnancy, “birth”, and bereavement have taken place. If there are remains to be buried as in the case of stillbirth, the loss can feel more complete and individuals spoke about having more control over their bodies and the outcomes if this was the case. For many, control and management of the miscarriage was a way in which management of the alienation that they felt could be handled. Specifically, many women in particular spoke of feeling ostracized from others, alienated from their bodies and at a loss as to how to explain the pregnancy loss. As Carol Byrnes said, “I felt as if I had done everything right, everything in my power and then I had none, no power, no ability to make sense of anything that had happened”. Amanda Brown offered a similar observation and said,
I was trying really hard to be healthy, take control over my diet, something that I never really did before, I was doing everything ‘right’ you know, really paying attention because I was aware enough of all the things that could go wrong and I was really worried this was genetic...I knew enough about what happened with my mom and grandma, this was something that they went through but nobody ever talked about. My mom was over and we were just sitting around talking one day and she brings this up, like all about her miscarriages and I’m was like ‘whoa, what? How come I never knew about this?’ and she said people just didn’t talk about it, there was nobody to talk to. So anyway I was really careful and my friend totally called me out, she saw me refusing coffee and not drinking and just having decaf or whatever and not going out....[laughs] it was hard to hide and I wasn’t even showing yet! Yeah but so I was trying hard to control when information got out, I was trying to control my body and in the end it just didn’t matter.
As Amanda noted and others discussed, the idea of failure and in particular of failed, overly medicalized bodies was present throughout the data.
Medicalization
For Karen Glazer, the way that the clinical personnel and hospital staff medicalized the miscarriage was disturbing. Not only was the miscarriage seen as a “failure” in clinical terms but the overly emotional nature of their traumatic experience led to very few interpersonal interactions with physicians or others who she felt “steered clear of the topic, it was just a procedure to them, nothing more” when she had returned for the D & C. For others too, the description and categorization of miscarriage as clinical (and individual) failure was pervasive in how they talked about loss and how they had begun to initially understand their pregnant body. Amanda Brown described how,
I was totally getting prepared for childbirth, I was online constantly, there are sites that will show you and tell you exactly how big your baby is at that moment, so some days I’d be at work and cruising around the internet and I’d think ‘oh, my baby is the size of a blueberry or chickpea’....it is kind of weird too, everything is about the size of a food [laughs] and it’s all very happy and benign and nothing is ever very clinical at all, it’s pretty happy and I’d say, maybe this is going to sound wrong, but it’s really presented nicely, it’s like women or people I guess are taught that being pregnant is something everyone can understand but not something that is ever negative or technical....its watered down and made ‘happy’...babies equal blueberries that sort of thing ....well all of that disappears when you miscarry...that “blueberry” becomes a “blighted ovum”, a “group of genetically mutated cells” or of course, the old standby...”your body’s mistake”....all very medical, all very technical.
Self-blame & isolation
Grace, a quiet woman in her mid-thirties spoke about her three miscarriages. One of Grace’s miscarriages occurred in her first marriage and she has had two more recently with her current marital partner. Grace’s story epitomizes the stigma and subsequent selfblame that many women (and men) experienced as a result of failed pregnancy. For Grace, her first miscarriage occurred when she and her first husband were young and newly married, as she described,
It took us by surprise for sure, I mean I’m not sure that we really wanted to have a baby then, we had been using birth control but not [laughs] very well I guess... So one day I was with my friend who was visiting and we were downtown, we had gone to an art show there I think, something free but that made us feel grown up you know? I was going to tell her during her visit about the pregnancy but hadn’t gotten that far when I had to go to the bathroom...I was cramping, agony.... worse than any period pains that I had ever even thought of, I think I knew what was happening to be honest, but I kept telling myself ‘oh maybe this is just part of pregnancy’...like it was something that I didn’t know about yet...wishful thinking. So I went to the bathroom and my friend followed me, I guess I didn’t look well, but she said she had to go too and we are side by side in the stalls, she asks me if I’m okay and I said finally ‘no, I’m having a miscarriage’....and just like that I’m crying and realizing how awful this is and I have to have it in the bathroom.
Numerous descriptions of the miscarriage experience illustrate how women feel to blame for the loss. In Grace’s case, she went on to describe how she felt that she had even caused it intentionally, “I had this thought that maybe I had wished it, that we weren’t ready, it was too soon and I had hoped for this outcome...I know that sounds silly, but I really had that idea that I had made it happen, I was really afraid that I just hadn’t wanted it enough”. Grace also described a response that many women noted, that she somehow “deserved” it and that the stigma associated with having a miscarriage was warranted. As she said,
I had an abortion when I was much younger, in my teens, I guess I thought that maybe that had caused the miscarriage, that first one anyway. I thought I was being punished...the funny thing is, we’re not at all religious, I didn’t grow up in a religious family really, we went to church occasionally but the punishment thing just came from me thinking about all the times I hadn’t wanted to get pregnant and then I was finally feeling happy about it and it felt like someone pulled the rug out from underneath my feet.
Again, Grace’s responses in interviews and discussions indicated the individual level of culpability that many who experience miscarriage describe. Other reasons that women gave for miscarriage as a direct result of their own behavior include: drinking too much coffee or consuming too much caffeine, working out too much, or getting “stressed out” at work and trying to “do too much”. All of these kinds of responses point to how women internalized and experienced miscarriage as a result of some individual transgression.
Keri Peterson spoke about the ways in which she felt that her miscarriage was her fault. She described both how she “was thrilled to find out about the pregnancy” but simultaneously “nervous because I wasn’t sure it was a good time for me to be having a baby”. Keri described how she continued to eat and drink whatever she typically did prior to finding out she was pregnant and said, “it included a lot of coffee...[laughs] I have times when I think that I should just have drunk a lot of coffee in my younger days because it seemed to prevent pregnancy from sticking...I could’ve avoided a lot of stupidity over getting the pill you know?” Keri blamed herself and her “coffee drinking habit” for her miscarriage and while there is some clinical evidence to suggest that caffeine intake can increase risk for miscarriage as a manifest explanation, the latent explanation, or the self-blame that Keri revealed, was a ubiquitous theme in all of the interviews. All individuals talked about how at some level they felt “to blame” for the pregnancy loss - either through their own actions or inattention to their bodies. As Keri put it, “I could never tell anyone just how much I felt it was my fault...at the hospital when I went that first time to make sure all the baby was gone, I basically felt like I was there for an abortion and everyone was judging me...they knew why I was there, but acted like it was my fault somehow for losing this baby”.
Men too talked about ways in which they felt miscarriage was their fault or they were to blame for failed pregnancies. Aaron, whose baby was stillborn said, “at the hospital we were pretty invisible, ignored totally...honestly it felt like we had some kind of disease and everyone, even the hospital staff was worried that it was catching”. Aaron also echoed the statements of other men and described feeling “responsible” when his wife was in pain, and for his lack of knowledge, “it is just hard to know what’s going on and I felt like I should have known more”.
Narratives of individual fault were reinforced in the language of others as well. Specifically, when others learned of a miscarriage, it was not uncommon to either deflect blame away or to create additional stigma. As Grace described,
So when I was having that first miscarriage, in that public bathroom and my friend is asking if I’m okay and yeah, yeah I was...it was gross and hurt but I was okay, it was probably still pretty early...anyway we left the art show and we were walking downtown along the river and my friend is just talking nonstop sort of and says ‘oh this happens to everyone I think’ and stuff like ‘oh you can try again right away’ and ‘I’m sure it just meant that that baby wasn’t going to be right’...like it was some kind of good thing...you know she might have been right but on the other hand that was not really what I wanted to hear...she just made it seem even more like my fault, like I was not very good at making a baby, I made a bad one and so she just dismissed it.
For many women and men, relatives’ responses echoed what Grace experienced. Todd, the partner of a participant, described how his mother responded when she’d heard that her daughter-in-law had had a miscarriage. He said, “she just kind of brushed it off, she said it happened to everyone and that we shouldn’t worry, it probably was meant to be, she said something about how a woman’s body always knows and just got rid of it”. For Todd and his wife and the myriad others who talked about the language of miscarriage this kind of response was typical. Perhaps not surprisingly however, very few ever talked about the experience of miscarriage outside of their most intimate relationships. Grace poignantly described how she thought that the problem of miscarriage “was just my problem, not a real problem or something that others would really want to know about, after a certain amount of time too, nobody, even those people who you tell, none of those people want to hear about it anymore...and there certainly aren’t any Hallmark cards at Krogers to send to someone who has a miscarriage”. Grace’s friend, Brittany Neel described how she and her husband got to the point where they were,
‘Faking infertility’ or problems getting pregnant because that was easier than trying to explain how many freaking times we ‘failed’ and had to mourn, exhausting to think about these as deaths you know, I think that is a protective mechanism in a sense, that I don’t allow myself to think too much about it. I don’t want to be one of those women who dwell so much on this - I just couldn’t take that, I don’t know who those people are, why do you want to celebrate those little deaths over and over again? I don’t get it.
Brittany also talked about the failure she felt that was symbolized in the material items that surround pregnancy. I think the hardest part for me was the clothing, the stuff - you know I wasn’t very pregnant yet and I sort of secretly bought a maternity dress...I mean secretly because I just ordered it from the Gap and it came online and nobody would know...I didn’t want to count chickens or jinx it somehow...maybe I was already worried, but anyway, I went ahead and bought this dress and it doesn’t really look all that different from other dresses, but I knew it was a maternity dress, so I hung it up and kept waiting, I was really excited to wear it and then the first miscarriage happened and then the second and now it’s just pushed to the back of the closet...I didn’t get rid of it yet, but some days I wonder how long I have to keep that damn dress...
In Grace’s case too, her subsequent miscarriages reinforced what she felt was the cultural assumption that women were most responsible as individuals for pregnancy losses even if those losses are due to environmental and less individual factors.
Environmental factors
Again, one of the themes that emerged was the tension between individual and environmental culpability. For many participants in this case study analysis, it was clear that while they did not necessarily feel “failure-free” in the sense that many (particularly women) reflected feelings of responsibility and failure akin to the descriptions that Karen Glazer gave for her problems becoming pregnant and the subsequent miscarriage; but rather that there were other factors that might be pinpointed as contributing to pregnancy loss. For Vanessa Nelson- Ramirez, who described herself as a Midwest native, environmental factors were the leading cause of her miscarriages in her mind.
Vanessa, she had just had her second miscarriage although this pregnancy had progressed further than her first. She felt extremely successful in many ways and said,
With this second pregnancy I did so many things correct...it is still a frustration, don’t get me wrong, I don’t want you to think I’m not upset about this, but I guess what I’d want people to know, the things that I didn’t know when I had my first miscarriage was all the stuff that you have to do to keep healthy and to keep everything around you healthy...I mean literally, like just not breathing in second-hand smoke made a huge difference I think, I got my boyfriend and his friends to quit, at least smoking in the house and car and I really think it made a difference. I read about how important vitamins are and now, as I’m thinking about taking baby aspirin to try again, that’s supposed to make it ‘stick’ somehow. I was also a lot more careful about what I ate, no fast food and in between I lost some weight, it is supposed to make it easier to get pregnant so I tried to just create a healthy me, a healthier environment for all of us and I think it worked, well....it worked to a point, now I have to figure out what else went wrong and try to fix that. For Vanessa, the understanding of the body as mechanical and as subject to external environmental factors was particularly salient. Hers was not the only narrative to describe the experience of miscarriage in these ways, many women talked about “fixing whatever was broken” and “making certain that the environment was healthy”. Even when there was disagreement over precisely what “healthy” meant in the focused and follow up discussions with women, most agreed that being “healthy” was inextricably linked to both individual and environmental behaviors and contexts. Individual explanations for miscarriage were less significant for those who talked about the role that environmental factors played.
While no women in this study had been exposed to radiation or had had chemotherapy of any sort, several pointed out that they were aware that exposures to chemicals and toxins of any kind (one woman worried about drinking from an old Nalgene water bottle made from BPA after she had a miscarriage) could lead to pregnancy loss and miscarriage in addition to birth defects among live children. Sarah O’Brien and her boyfriend Tyler Moore both mentioned awareness of how environment and health were related in terms of pregnancy outcomes. Sarah, a high school graduate who is working while taking courses at the local community college in preparation for nursing school described how “people are more aware of the way what we do to the environment can affect our health, I don’t think that is surprising, but when I was pregnant I was suddenly way, way more aware of breathing in smoke, or pollution or [laughs] I became one of those people who actually read nutrition labels!” Tyler confirmed a similar shift in his perception of the environment, “I learned about toxins in school [college] and was always aware of that stuff, how bad it can be for you but when Sarah was pregnant we even got the app so you can click on a food and see what’s in it.”
Provider perspectives
Medicalized bodies: Provider perspectives on the experience of miscarriage highlighted several themes that intersected in various ways with the meanings that individuals gave to the experience. Specifically, providers spoke in gendered ways about miscarriage and reinforced the idea of body as machinery and as something to be fixed, maintained and repaired. Several providers noted too that despite their frustration that patients were not aware of the frequency of miscarriage across the population, they were unwilling to talk about the possibility or potential of miscarriage, or pregnancy complications with their patients; often deflecting questions during initial, routine pre-natal visits and suggesting that “typically patients do not want to hear the negative, the possible bad stuff, we are way more accustomed to focus on the positive and not on the realistic”. Overall provider perspectives suggested both individual and environmental factors were to blame for miscarriage. As Kerry Maynard, a self-described “rural doctor through and through” and someone who finally found her role in being able to care and spend time with underserved populations, noted, “a lot of times I wish I had pointed out the potential problems, the things that can go wrong and the ways to be careful during pregnancy”. Kerry is an ob/gyn who sees a great deal of the women in Putnam County. She moved to the area over ten years ago and as her reputation for being a caring doctor has grown, so has the waiting list to become one of her patients. Kerry talked about how she was taught to think about miscarriage and pregnancy loss in medical school and reflected some of the same themes that patients such as Grace Kaufmann and others highlighted. Kerry described, When I was in school you pretty much learned about the weeks of gestation, what happens when and the nuts and bolts of fetal development. We learned about hormone levels and at the time the hot thing to study was fetal alcohol syndrome so we were all pretty immersed in learning about that...but now that I think about it, so much of what we were taught was about the problems that patients brought onto themselves, their behaviors and that miscarriage was a kind of ‘natural’ outcome of some of these things.
For Kerry, it became clear that with the rise of assisted reproductive technologies, wealthier women too were the ones who would increasingly have access to healthy and successful reproductive outcomes in ways that those with fewer socio-economic advantages did. For her, working as a health care provider, the issue of miscarriage is inextricably linked to cultural and demographic factors that affect fertility outcomes. She said, “one of the hardest things here is to convince people to eat more healthily, to reduce sugar in the diet and sodas...oh my god...don’t get me started on coke sizes and refills...diabetes, keeping a healthy weight and no tobacco, those are the things I emphasize” she said. But in rural Indiana, numerous women who Kerry attended to and saw throughout their pregnancies or miscarriages did not have the financial resources or easy access to better food options. Importantly however, when thinking about provider perspectives on the management and medicalization of miscarriage, no provider spoke of miscarriage or pregnancy loss as something other than an individual level, or personal problem. In fact, one provider argued that, “miscarriage is just not a public health problem, there is no way you are going to make people believe that not being able to have children or keep a pregnancy is on the same playing field as AIDS or the flu.” While others provided more nuanced insight, suggesting for example that larger structural inequalities in women’s health and the value of feminist perspectives could help illuminate the reasons for neglect of miscarriage in the field, and into how and why miscarriage might not be seen as a public health problem. Miscarriage is cast as “failure”, as one physician put it, “as amped up menstruation, the body is just getting rid of unwanted, unusable material” and such assumptions can potentially influence policy or attention and funding given to dissemination of information or care and support to those who suffer miscarriage. The physician’s statement above is an important reflection on assumptions about where funding and public health education and information are disseminated in general and with respect to pregnancy loss in particular.
While Kerry Maynard recognized the significance of the sociocultural and environmental factors that influenced miscarriage, she readily admitted that she was, “still wedded to that medical model...I really have a hard time talking about miscarriage as something other than reproductive failure or to use terms like ‘blighted ovum’ when I’m trying to explain what happened”. Kerry echoed precisely what patients such as Karen and Steven experienced and reinforced the notion that the language of miscarriage is grounded in medical, technical and mechanical metaphors. For Kerry too, she described the desire on her part to reassure her patients that in fact miscarriage was common and perhaps not the devastating news they so often assumed. She stated that “I know it is difficult, no doubt about it, but I at least try to remind women, and men too I guess, that miscarriage happens a lot, it is just that people don’t go talking about it that much...most people go on to have successful pregnancies”. She spoke on several occasions about the need to improve her own provider practices and to include some acknowledgement of the potential for miscarriage in early pregnancy. As she put it however, “I think I’m just hesitant to talk about it, loath to talk about it really, because I have this fear that if I talk about it, it will jinx the pregnancy, the patient will think I had something to do with it and I’ll lose their trust.”
Trust and control: Trust is an essential part of John Foulkes’ narrative about himself. As a physician who has long practiced in Indiana, Kentucky and Michigan, John described himself as someone who has had a “good deal of experience” with the experience of pregnancy and loss and added “miscarriage should be seen as just part and parcel of pregnancy, but nobody ever wants to hear that, no patient wants to talk about it.” John has had an unique approach to talking to patients about miscarriage - he encourages them to talk candidly with him about the experience and he is a vehement critic of the language used to describe miscarriage as anything other than clinical. By this he means that both patients and physicians should be using language that describes precisely what is going on, insisting on as he said, “correct medical terminology” and he is an avid critic of popular culture and magazines that “focus on that damn culture of the baby bump but never say a word about the speed bumps along the way.” John believes that patients should be empowered with knowledge about their experience but his own narratives suggest that that experience is a largely clinical one. As he puts it, [I want patients to know what is going on in their own body...it is not mystical, it’s not magic, it is science and there are things that can be done to control that science and the outcomes, just like any other experiment I guess and that makes it an easy way to explain what happened to a lot of these women. I tell them not to smoke, don’t drink, eat good food and take vitamins and that things will work out].
While John’s explanation at times echoes the blame and deflection that Vanessa and Todd experienced, John argued that it was not about “lessening” the experience of miscarriage, but trying to actively teach women about their bodies and help inform others as to what to do to have a healthier outcome. John is known in his practice and in the reproductive health community nearby for suggesting to women and their partners that it might be useful and informative to collect the products of miscarriage in order to learn (if patients bring the fetal product to him he will help them look at it and discuss it, he will even give one instructions about how to collect blood and material from the toilet without contaminating the ‘specimen’) about the reproductive process.
Not all providers in all communities around the country or globe are like John in his straightforward use of clinical language and followup with individual patients and families. For the most part when asking women and men about their experiences with providers during or after a miscarriage, most suggested that they prefer that their providers were not “so involved” and most noted that their care providers did not have much interaction at all.
As Jodi, a woman who had just had her third miscarriage said, “they [physicians] just expect you to dust yourself off, pick up and start all over again, it’s like they want to get it right and so they expect that you want the same thing...sometimes it is exhausting...I had days where I felt like a puppy mill but without the puppies...” Others noted too that the kind of “over-involvement” or “attention” that their miscarriages received just served to heighten the sense that they (the patient) were to blame. As Jodi continued, “I kept feeling like I was being coached, if I just kept practicing enough, I’d finally get it right and then everyone would be pleased with my work”.
For John and other providers however, the idea of “fixing” or having control over the reproductive body was paramount. From the language he chose to use to the emphasis he placed on empowerment of patients, John was a good example of provider perspectives on pregnancy loss, I’d say the hardest part about having to do a D & C after a miscarriage, if it’s not a clean miscarriage, a natural one, is that feeling that you are actually performing an abortion...don’t get me wrong, I’m pro-choice, I have grown daughters, I have always wanted them to be have a choice over their bodies...control...but when you are actually performing this action, something they teach you in medical school...all of a sudden there’s this conflict, at least if you are a thinking physician, if you are paying attention to what you are doing and how complex a moment that is...the same is true when I have to tell a woman and her husband or boyfriend about the process of miscarriage...I can get tongue tied, even when I insist on using the ‘right’ language.
A sense of control and of miscarriage as something devoid of any politicized or problematic emotions is something that John and other providers (both male and female) expressed.
Discussion
There is limited recognition of the ubiquity of miscarriage in reproductive life in the contemporary (and particularly rural) U.S. contexts. Increasingly, in a world with ever-shifting fertility technologies to help people fulfill reproductive desires, the idea of control over reproductive “failures” in particular has come into sharp relief. Yet the meaning and management of miscarriage remains stunted in relative comparison to other aspects of reproductive life. It remains shrouded from both everyday public as well as scientific discourse [3,5,10]. Literature and popular culture have acknowledged that pregnancy loss may cause emotional distress, discomfort and offer a challenge to family building and planning but rarely are ethnographic investigations of the experience conducted or the cultural meaning of miscarriage explored. At the same time the majority of Americans inaccurately believe miscarriage is rare and misunderstand its causes, creating an often isolating and guilt-ridden experience for those who experience it. Given that miscarriage is a traditionally taboo subject for many, it is not surprising that the meanings of miscarriage for both patients and providers have long been seen as individual rather than public health concerns. Overwhelmingly patients and providers emphasized the necessity for increased awareness of actual versus perceived health risks as related to miscarriage, increased communication about miscarriage (in both public and private spheres) as well as preparation for any future potential pregnancy. This study offers practical outcomes given the implications of these findings for other studies of reproductive health.
Utility of theoretical framework
This study used the socio-ecological systems theory to understand the lived experiences, perceptions of risk and the management of miscarriage in the everyday lives of individuals and their providers. Such a theory posits that behavior and experience is understood through the various and integrated levels of interaction between individuals, family, organizations and communities. Thus, an individual who is grappling with a miscarriage is immersed in networks that will influence their reaction to the perceived risk factors, experience and in managing the outcomes of the experience. Throughout this study participants discussed the strengths and limitations of interactions in each of these realms. Individual responses to or understandings of the potential risks of miscarriage were raised by all participants, from women who had the experience, their partners as well as in discussion with providers. At another level, the experience of and perceptions of miscarriage were discussed with others in support groups, amongst friends and colleagues to a limited degree and these discussions (or lack thereof) affected opinions about the relative invisibility that surrounds the experience. Broader attitudinal factors and cultural as well as institutional attention to miscarriage were an additional level of interaction for participants. A key aspect to this theoretical model is that it suggests that individuals in these myriad, intertwined social realms are able to adapt to changing norms, policies and influential factors. For those in this study this was certainly the case. Participants talked about understanding the need to control risks, increase health literacy, find formal or informal support groups as well as the need to increase discussion about this oftenoverlooked health experience, both between partners as well as patients and providers.
As patients and provider narratives highlighted particular themes such as control over the body, gender and the medicalization of birth, it was clear that miscarriage was not simply an individual level result, but rather, that it was the product of multiple influences. Given this, it is possible to understand how better support systems and considerations of gender and power in reproductive care can vastly improve outcomes for patients.
Conclusion
This study illuminates the perceptions and experiences of risk associated with having a miscarriage among women in the rural Midwest who experienced at least one miscarriage. The experience of miscarriage is relatively undiscussed in public health literature. Patient providers and partners of participants were also interviewed and add to the findings about how those who experience miscarriage make meaning of the risks associated with pregnancy loss. By learning how these women and their partners/providers made meaning of their perceptions of risk as well as the experience of miscarriage within the context of their environment, public health practitioners will have a more comprehensive understanding of the impact of miscarriage on perceptions of relationships, family status and reproductive health in under-resourced settings.
Participants highlighted concepts of control, over-medicalization and the machination of the body. They discussed gendered aspects of blame and individual as well as environmental culpability. They speculated on individual versus broader cultural narratives and messages that are received in U.S. society on the meaning of miscarriage and compared their own lived experiences to the popular understandings (or misunderstandings as the case may be) about pregnancy loss.
In order to achieve better patient care and women’s reproductive health care in particular, attention to seemingly individual level experiences such as miscarriage must be paid. Miscarriage must be understood not simply as a facet of individual health beliefs or behaviors but rather in terms of greater public health concerns, social inequalities and gender expectations, aspects of the socio-cultural environment. It will be essential for patients, providers and partners to recognize the salience of the range of perspectives on miscarriage and for additional qualitative, exploratory studies such as this one to be completed. Results will have implications for research, practice, and personal health care in multiple contexts.
Declaration of Competing Interests
The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support with respect to the research, authorship, and/or publication of this article.
References
- Lerner H (2003) Miscarriage: Why it happens and how best to reduce your risks. Massachusetts: Perseus Publishing.
- McCreight BS (2004) A grief ignored: Narratives of pregnancy loss from a male perspective. Sociology of Health & Illness 26: 326-350.
- Cecil R (1996) The anthropology of pregnancy loss: Comparative studies in miscarriage, stillbirth and neonatal death. Berg.
- Murphy F, Philpin S (2010) Early miscarriage as “matter out of placeâ€: An ethnographic study of nursing practice in a hospital gynaecological unit. Int J Nurs Stud 47: 534-541.
- Darney BG, Weaver MR, Derhei VD, Stevens NG, Prager SW (2013) “One of those areas that people avoid†a qualitative study of implementation in miscarriage management. BMC Health Serv Res 13: 123.
- Swanson KM (1999) Effects of caring, measurement, and time on miscarriage impact and women’s well-being. Nursing Research 48: 288-298.
- Swanson KM, Chen HT, Graham JC, Wojnar DM, Petras A. Resolution of depression and grief during the first year after miscarriage: A randomized controlled clinical trial of couples focused interventions. J Womens Health (Larchmt) 18: 1245-1257.
- Jansson C, Adolfsson A (2011) Application of “Swanson’s middle range caring theory†in Sweden after miscarriage. Inter J Clin Med 2: 102-109.
- Abboud L, Liamputtong P (2005) When pregnancy fails: Coping strategies, support networks and experiences with health care of ethnic women and their partners. J Reprod Infant Psychol 23: 3-18.
- Marcia I (2007) Reproductive disruptions: Gender, technology, and biopolitics in the new millennium. Berghan Books: Oxford.
- Reagan, Leslie J (2003) “From hazard to blessing to tragedy: Representations of miscarriage in twentieth-century America.†Feminist Studies 9: 356-378.
- Macaluso M, Wright-Schnapp TJ, Chandra A, Johnson R, Satterwhite CL, et al. (2010) A public health focus on infertility prevention, detection, and management. Fertil Steril 93: e1-e10.
- Brady G, Brown G, Letherby G, Bayley J, Wallace LM (2008) Young women’s experience of termination and miscarriage: A qualitative study. Hum Fertil (Camb) 11: 186-190.
- Simmons RK, Singh G, Maconochie N, Doyle P, Green J (2006) Experience of miscarriage in the UK: Qualitative findings from the National women’s health study. Soc Sci Med 63: 1934-1946.
- Smith LF, Frost J, Levitas R, Bradley H, Garcia J (2006) Women’s experiences of three early miscarriage management options: A qualitative study. Br J Gen Pract 56: 198-205.
- Rajan L, Oakley A (1993) No pills for heartache: The importance of social support for women who suffer pregnancy loss. J Reprod Infant Psychol 11: 75-87.
- Rowlands IJ, Lee C (2010) “The silence was deafeningâ€: Social and health service support after miscarriage. J Reprod Infant Psychol 28: 274-286.
- Christine GA, Braun B (2017) Single female breast cancer patients’ perspectives on intimate relationships. Qual Health Res 27: 1461-1472.
- Harris LH, Dalton VK, Johnson TRB (2007) Surgical management of early pregnancy failure: History, politics, and safe, cost-effective care. Am J Obstet Gynecol 196: e1-e5.
- Cecil R (1994) Miscarriage: Women’s views of care. J Reprod Infant Psychol 12: 21-29.
- Root R, Browner C (2001) Practices of the pregnant self: Compliance with and resistance to prenatal norms. Cult Med Psychiatry 25: 195-223.
- De La Rochebrochard E, Thonneau P (2002) Paternal age and maternal age are risk factors for miscarriage; Results of a multicentre European study. Hum Reprod 17: 1649-1656.
- Kleinman A (1989) The illness narratives: Suffering, healing and the human condition. Basic Books.
- Triche EW, Hossain N (2007) Environmental factors implicated in the causation of adverse pregnancy outcome. Seminars in Perinatology 31: 240-242.
- Bansen S, Stevens H (1992) Women’s experiences of miscarriage in early pregnancy. J Nurse Midwifery 37: 84-90.
- Small ML (2009) How many cases do I need? On science and the logic of case selection in field-based research. Ethnography 10: 5-38.
- http://www.yanchukvladimir.com/docs/Library/Sage%20Encyclopedia%20of%20Qualitative%20Research%20Methods-%202008.pdf
- Creswell JW (1998) Qualitative inquiry and research design: Choosing among five traditions. London: Sage.
- Patton M (2014) Qualitative research methods. Thousand Oaks: Sage publications.
- Layne L (2002) Motherhood lost: A feminist account of pregnancy loss in America. Routledge.
- Weng X, Odouli R, Li DK (2008) Maternal caffeine consumption during pregnancy and the risk of miscarriage: A prospective cohort study. Am J Obstet Gynecol 198: e1-e8.
Citation: Rebecca LU (2019) Perceptions of Miscarriage among Patients and Providers: Risk, Management and Control of the Body. J Comm Pub Health Nursing 5:224. DOI: 10.4172/2471-9846.1000224
Copyright: © 2019 Rebecca LU. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Select your language of interest to view the total content in your interested language
Share This Article
Recommended Journals
Open Access Journals
Article Tools
Article Usage
- Total views: 3717
- [From(publication date): 0-2019 - Dec 07, 2025]
- Breakdown by view type
- HTML page views: 2855
- PDF downloads: 862