Complications and Mortality after Major Amputation in Patients with Critical Limb Ischemia: A Single Center Experience
Received: 02-Jan-2019 / Accepted Date: 30-Jan-2019 / Published Date: 06-Feb-2019
Abstract
Objectives: Patients with critical limb ischemia (CLI) and undergoing major lower limb amputation carry a high risk of perioperative morbidity and mortality. This paper described complications and mortality rates in the short and long term after major amputation in patients with CLI and analyzed the preoperative comorbidities for predicting postoperative outcomes.
Methods: From January 2004 to March 2017, 140 consecutive major lower extremity amputations were performed in patients affected by CLI. Preoperative comorbidities associated with perioperative complications and mortality after lower extremity amputation were identified and analysed.
Results: Complication rate was 20%. There was a confirmed association between perioperative complications and congestive heart failure (OR 2.8, p=0.02), chronic obstructive pulmonary disease (COPD) (OR 0.3, p=0.02) and hypertension (OR 10.5, p=0.02). In-hospital mortality rate was 26.4% (n=37), 28.4% (n=31) of above-knee amputation (AKA) patients and 19.3% (n=6) of below-knee amputation (BKA) (p=0.3). Congestive heart failure was also significantly associated with in-hospital mortality (OR 2.3, p=0.04). Survival at 1, 2 and 5 years was 61.6%, 58.1% and 39.3% respectively. Advanced age was significant predictor of mortality (OR 3.8, p=0.001). Survival at 1, 2 and 5 years in AKA group was 53.3%, 50.2% and 33.3% respectively compared with BKA group in which survival at 1, 2 and 5 years was 88%, 83.1% and 58.2% respectively (p=0.004).
Conclusions: Nowadays, major amputation remains associated with high complication and mortality rates; some comorbidities seem to be associated with these outcomes.
Keywords: Amputation; Critical limb ischemia; Peripheral artery disease
Introduction
Despite advances in medicine and surgical area, major lower limb amputation is still a worldwide problem. Peripheral arterial disease, at the stage of critical ischemia, leads to amputation within a year in 30% of cases [1]. This intervention is obviously reserved to those cases when endovascular or surgical revascularization is not possible or unsuccessful. Numerous studies over the last 30 years have proven that the major amputation of the lower limb is associated with a high mortality in the short and long term, as well as a high incidence of local and systemic complications [2-4].
Our study is aimed to analyze perioperative complications and mortality after major amputation in patients affected by critical limb ischemia (CLI). The objective of this study is also to investigate the relationship between patient comorbidities and postoperative outcomes.
Material and Methods
The study was based on a retrospective analysis of prospectively collected data. All patients who underwent major lower extremity amputations, from January 2004 to March 2017, were identified. The analysis was limited to above–knee (AKA) and below–knee amputations (BKA) performed for vascular disease, major amputations resulting from trauma, cancer and infection were excluded. Demographic and clinical data, procedural information and postoperative complications (level of amputation, reamputation and perioperative mortality) were collected.
Categorical variables were presented as frequencies with percentages and continuous variables as means with SDs. Comparisons of categorical data were pursued with χ2 and Fisher exact tests. Comparisons of nonparametric continuous data were investigated using the Mann-Whitney U test. Multivariate analysis was run using logistic regression to identify variables associated with perioperative complications, reintervention, and perioperative mortality. Multivariate model was fit for variables that were marginally associated with outcomes on univariate analysis (p<0.1). Level of association was described in odds ratios (ORs) with 95% confidence intervals (CIs). Kaplan-Meier estimates of survival were calculated at 1, 2 and 5 years. Level of association was described in hazard ratios (HRs) with 95% confidence intervals (CIs). p values<0.05 were considered significant. Analysis was performed using IBM SPSS (SPSS, Chicago, Ill).
Results
One hundred forty consecutive major lower extremity amputations were performed during the study period in patients affected by CLI. Patient demographics and comorbidities are listed in Table 1. The mean age was 74.8 ± 10.9 years. The majority of cases were men (66.4%) and former or current smokers (56.5%). At the time of enrolment, 114 patients (81.4%) had a history of hypertension, 91 patients had hyperlipidemia (65%) and 92 patients suffered from diabetes (65.7%). Ninety-one patients (65%) underwent ipsilateral lower extremity procedure previously. These data were displayed in Table 1. Of the 140 amputations performed, 31 (22.1%) were transtibial amputation and 109 (77.9%) were transfemoral one (Table 1). The median (25th, 75th percentile) length of stay was 13 days (7 days, 22 days). All perioperative complications are reported in Table 2. Complication rate was 20% (n=28). Nine (39.1%) of 23 cases of wound dehiscence required a conversion to a higher-level amputation (3 above-knee amputation and 6 coxofemoral hindlimb disarticulation). The relationships between comorbidities and perioperative complications are examined. They are summarized in Table 3. Hypertension, chronic obstructive pulmonary disease (COPD), congestive heart failure and myocardial infarction were selected for multivariate analysis. There was a confirmed association between perioperative complications and congestive heart failure (or 2.8, p=0.02), COPD (or 0.3, p=0.02) and hypertension (or 10.5, p=0.02). In-hospital mortality rate was 26.4% (n=37), 28.4% (n=31) of AKA patients and 19.3% (n=6) of BKA one (p=0.3). Univariate analysis of factors associated with in hospital mortality was performed (Table 4) and among these factors, congestive heart failure was significantly associated with this outcome (or 2.3, p=0.04). No significant association was observed between level of amputation and in-hospital mortality.
| Variable | Level | n | % |
|---|---|---|---|
| Gender | Male | 93 | 66 |
| Age (years) | 74.8 ± 10.9 | ||
| Smoking | Former smoker | 40 | 29 |
| Current smoker | 39 | 28 | |
| Hypertension | 114 | 81 | |
| Hyperlipidemia | 91 | 65 | |
| Diabetes mellitus | 92 | 66 | |
| COPD | 51 | 36 | |
| Renal insufficiency | 33 | 24 | |
| Myocardial infarction | 46 | 33 | |
| Congestive heart failure | 52 | 37 | |
| Cerebral vascular insufficiency | 19 | 14 | |
| Pre-amputation procedures | 91 | 65 | |
| PTA/Stenting | 30 | ||
| Bypass | 44 | ||
| Pedal amputation | 18 | ||
| Other | 20 | ||
| Index amputation level | BKA | 31 | 22 |
| AKA | 109 | 78 | |
COPD: Chronic Obstructive Pulmonary Disease; PTA: Percutaneous Transluminal Angioplasty; BKA: Below Knee Amputation; AKA: Above Knee Amputation
Table 1: Patient demographics, comorbidities and procedure details.
| BKA n (%) | AKA n (%) | ||
|---|---|---|---|
| Total n=31 | Total n=109 | p Value | |
| In-hospital death | 6 (19.3) | 31 (28.4) | 0.3 |
| Complications | 7 (22.6) | 21 (19.3) | 0.7 |
| Debridement | 2 (28.6) | 11 (52.3) | |
| Reintervention | |||
| Above-knee amputation | 3 (42.8) | / | - |
| Coxofemoral hindlimb disarticulation | / | 6 (28.6) | |
| Treatment with VAC-Therapy | 1 (14.3) | / | |
| Massive pleural effusions | - | 1 (4.8) | |
| CAP | 1 (14.3) | 1 (4.8) | |
| Acute pulmonary edema | - | 2 (9.5) | |
VAC: Vacuum Assisted Closure; CAP: Community Acquired Pneumonia
Table 2: Postoperative complications.
| Factor | Univariate OR (95% CI) | p Value |
|---|---|---|
| Age >75 | 0.8 (0.4-2) | 0.7 |
| Male gender | 0.9 (0.4-2.1) | 0.8 |
| Hypertension | 7.7 (1-60) | 0.05 |
| Smoking | 0.6 (0.3-1.4) | 0.2 |
| Hyperlipidemia | 1.8 (0.7-4.6) | 0.2 |
| COPD | 0.3 (0.1-0.9) | 0.03 |
| Congestive heart failure | 2.3 (1-5.4) | 0.04 |
| Myocardial infarction | 0.5 (0.2-1.3) | 0.1 |
| Diabetes | 0.8 (0.3-1.8) | 0.5 |
| Renal insufficiency | 0.8 (0.3-2.3) | 0.7 |
| Cerebral vascular insufficiency | 1 (0.3-3.5) | 0.9 |
COPD: Chronic Obstructive Pulmonary Disease
Table 3: Patient demographics, comorbidities and perioperative complications.
| Factor | Univariate OR (95% CI) | p Value |
|---|---|---|
| Age >75 | 1.4 (0.7-3) | 0.3 |
| Male gender | 0.7 (0.3-1.7) | 0.5 |
| Hypertension | 0.6 (0.2-1.5) | 0.3 |
| Smoking | 1.2 (0.5-2.5) | 0.6 |
| Hyperlipidemia | 0.8 (0.4-1.8) | 0.7 |
| COPD | 0.8 (0.3-1.7) | 0.5 |
| Congestive heart failure | 2.2 (1-4.8) | 0.04 |
| Myocardial infarction | 0.8 (0.3-1.8) | 0.6 |
| Diabetes | 0.6 (0.3-1.3) | 0.2 |
| Renal insufficiency | 1.9 (0.8-4.3) | 0.1 |
| Cerebral vascular insufficiency | 1.8 (0.6-4.9) | 0.3 |
| AKA | 1.6 (0.6-4.4) | 0.3 |
COPD: Chronic Obstructive Pulmonary Disease; AKA: Above Knee Amputation
Table 4: Patient demographics, comorbidities and in-hospital mortality.
The median (25th, 75th percentile) follow-up was 16 months (3 month, 47 months). Survival at 1, 2 and 5 years was 61.6%, 58.1% and 39.3% respectively (Figure 1). Univariate analysis revealed that only age (OR 3.8, p=0.001) was significant predictor of mortality. It was calculated long-term survival stratified by amputation level (Figure 2). Survival at 1, 2 and 5 years in above-knee amputation group was 53.3%, 50.2% and 33.3% respectively, compared with below-knee amputation group, in which survival at 1, 2 and 5 years was 88%, 83.1% and 58.2% respectively (p=0.004). Comparing preoperative characteristics that could justify this result, the advanced age was statistically significant in patients underwent transfemoral amputation (p=0.04).
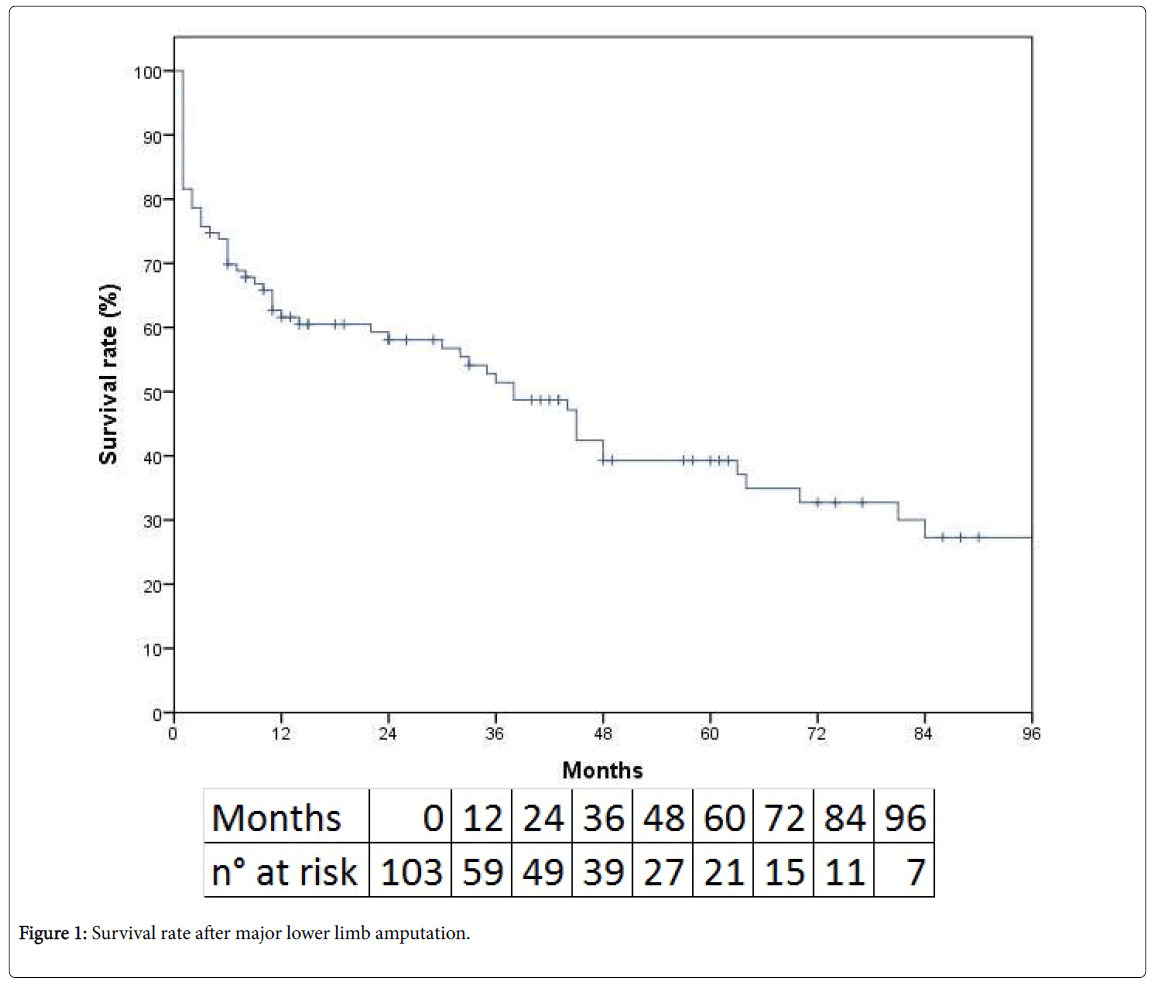
Figure 1: Survival rate after major lower limb amputation.
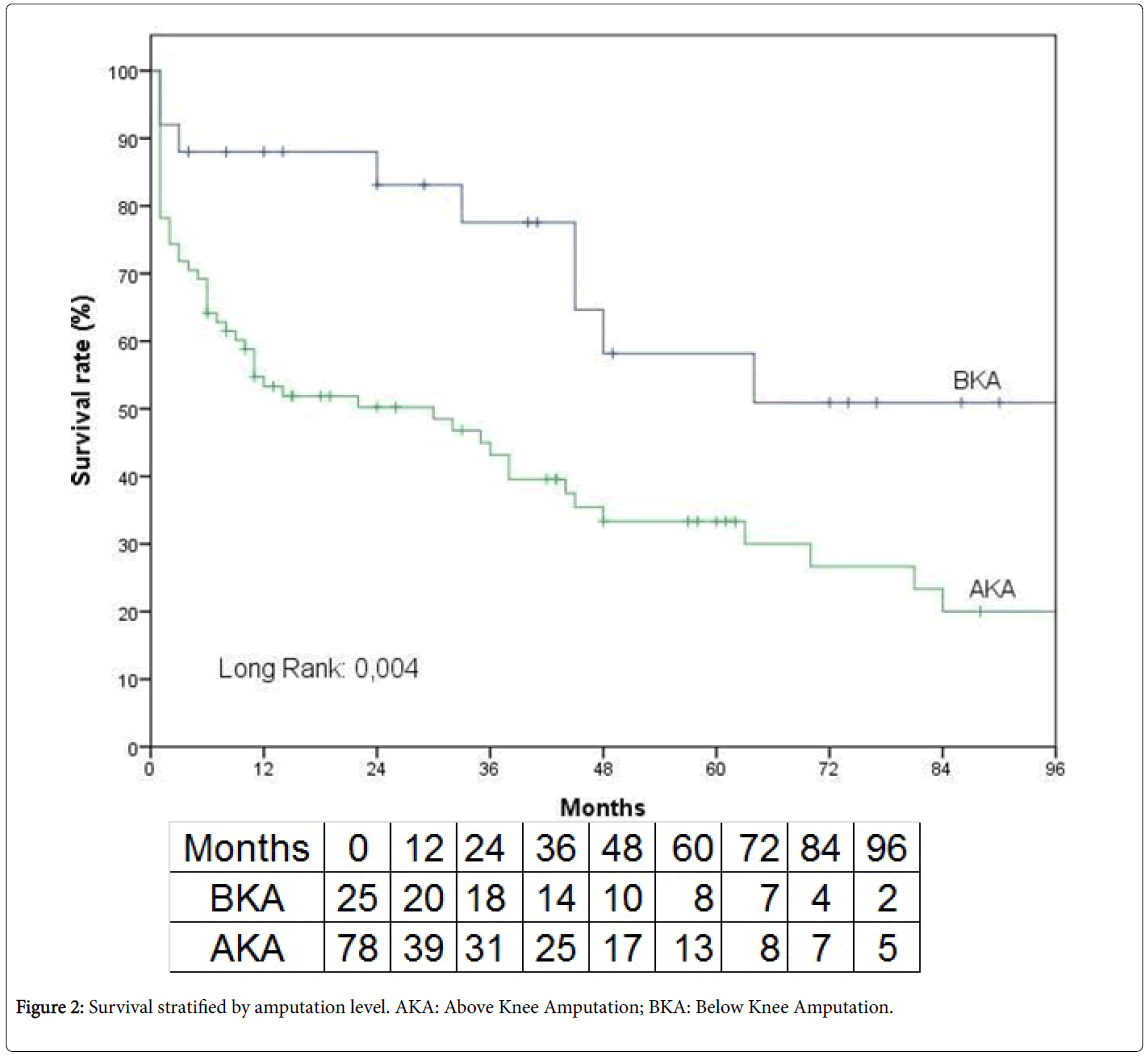
Figure 2: Survival stratified by amputation level. AKA: Above Knee Amputation; BKA: Below Knee Amputation.
Discussion
CLI is associated with high mortality rates of up to 25% after 1 year and up to 64% after 4 years [5,6]. Major amputation is indicated when any other therapeutic option has failed or gangrene and/or infection are too spread. Survival rates after major amputation in patients with CLI are limited [7,8]. Stratifying the level of major amputation, Malone et al. described a higher mortality in patients underwent to above-knee amputation (20%-40%) than patients with below-knee amputation (3%-10%) [9]. Literature has emphasized a high rate of perioperative complications after major amputation. According to a multicentre study, only 42% of the stumps recovered without complications [10]. In a review of Dormandy et al. 20% of transtibial amputation, 22% of disarticulation of the knee and 8% of the transfemoral amputations had revisioned or underwent a reamputation [4]. Other studies suggest that the primary healing of below-knee amputations varies between 30 and 92% and that the number of reamputations varies between 4% and 30% [11]. In the work of Dillingham et al. reamputation rates were approximately 19.7% for the BKA and 12% for the AKA [12]. In the present study, postoperative complications rate was 20% with a reamputation rate of 6.4%. Congestive heart failure, COPD and hypertension were also reported to have an adverse effect on perioperative complications.
According with scientific literature, it can be assumed that a lower level of amputation offers major advantages in terms of perioperative mortality but fewer advantages in terms of number of reamputations [4,12,13]. The analysis proved to be in accordance with the literature, showing a high rate of mortality during follow up; survival at 1, 2 and 5 years was respectively 61.6%, 58.1% and 39.3%.
In some studies, more than 50% of the patients died after 2 years and 70% after 5 years [14,15]. Fortington et al. showed a mortality at 30 days of 22%, at 1 year of 44% and at 5 years of 77% [16]. Multiple studies found significant relationships between risk factors and composite adverse outcomes in patients with CLI who underwent to major amputation. As a matter of fact, advanced age, COPD, dialysis and high cardiologic risk are associated with significant increase of mortality [17]. In this study, age over 75 years was as a remarkable risk factor for mortality.
Although diabetes mellitus is associated with a high risk of major amputation, the present analysis did not find, in agreement with other studies, significant association with mortality risk [13,18-21].
Level of amputation was associated with increased long-term mortality. This data is in agreement with a retrospective study of Aulivola et al. the overall survival was 69.7 % and 34.7% at 1 and 5 years, respectively. Survival was worse for above-knee amputations (50.6% and 22.5%) than below-knee amputations (74.5% and 37.8%) [22].
Conclusions
Despite the endovascular and surgical techniques improve perfusion in patients with CLI, in many instances, the major amputation remains the only surgical option. At present, major amputation remains associated with high complication and mortality rates and some comorbidities seem to be associated with these outcomes.
References
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, et al. (2007) Inter society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg 45: S5-67.
- Klaphake S, De Leur K, Mulder PG, Ho GH, de Groot HG, et al. (2017) Mortality after major amputation in elderly patients with critical limb ischemia. Clin Interv Aging 12: 1985-1992.
- Fang ZB, Hu FY, Arya S, Gillespie TW, Rajani RR (2017) Preoperative frailty is predictive of complications after major lower extremity amputation. J Vasc Surg 65: 804-811.
- Dormandy JA, Ray SA (1994) The fate of amputees. Vasc Med Rev 1995: 331-346.
- Catalano M (1993) Epidemiology of critical limb ischaemia: North Italian data. Eur J Med 2: 11-14.
- Reinecke H, Unrath M, Freisinger E, Bunzemeier H, Meyborg M, et al. (2015) Peripheral arterial disease and critical limb ischaemia: Still poor outcomes and lack of guideline adherence. Eur Heart J 36: 932-938.
- Dormandy JA (1992) Natural history of patients with peripheral occlusive arterial disease. Ann Chir Gynaecol 81: 86-88.
- Pell J, Stonebridge P (1999) Association between age and survival following major amputation. The scottish vascular audit group. Eur J Vasc Endovasc Surg 17: 166-169.
- Malone JM (2002) Lower extremity amputation. In Moore W Vascular surgery: A comprehensive review. 6th edn. WB saunders company, Philadelphia.
- Dormandy JA, Belcher G, Broos P, Eikelboom B, Laszlo G, et al. (1994) Prospective study of 713 below-knee amputations for ischaemia and the effect of a prostacyclin analogue on healing. Br J Surg 81: 33-37.
- Dormandy J, Heeck L, Vig S (1999) Major amputations: Clinical patterns and predictors. Semin VascSurg 12: 154-161.
- Dillingham TR, Pezzin LE, Shore AD (2005) Reamputation, mortality, and health care costs among persons with dysvascular lower-limb amputations. Arch Phys Med Rehabil 86: 480-486.
- Karam J, Shepard A, Rubinfeld I (2013) Predictors of operative mortality following major lower extremity amputations using the national surgical quality improvement program public use data. J Vasc Surg 58: 1276-1282.
- De Luccia N, Pinto MA, Guedes JP, Albers MT (1992) Rehabilitation after amputation for vascular disease: A follow-up study. Prosthet Orthot Int 16: 124–128.
- Nehler MR, Coll JR, Hiatt WR, Regensteiner JG, Schnickel GT, et al. Functional outcome in a contemporary series of major lower extremity amputations. J Vasc Surg 38: 7-14.
- Fortington LV, Geertzen JHB, van Netten JJ, Postema K, Rommers GM, et al. Short and long term mortality rates after a lower limb amputation. Eur J Vasc Endovasc Surg 46: 124-131.
- Shah SK, Bena JF, Allemang MT, Kelso R, Clair DG, et al. (2013) Lower extremity amputations: Factors associated with mortality or contralateral amputation. Vasc Endovascular Surg 47: 608-613.
- Suckow BD, Goodney PP, Cambria RA, Bertges DJ, Eldrup-Jorgensen J, et al. (2012) Predicting functional status following amputation after lower extremity bypass. Ann Vasc Surg 26: 67-78.
- Jones WS, Patel MR, Dai D, Vemulapalli S, Subherwal S, et al. (2013) High mortality risks after major lower extremity amputation in medicare patients with peripheral artery disease. Am Hearth J 165: 809-815.
- Bates B, Stineman MG, Reker DM, Kurichi JE, Kwong PL (2006) Risk factors associated with mortality in a veteran population following transtibial or transfemoral amputation. J Rehabil Res Dev 43: 917–928.
- Schofield CJ, Yu N, Jain AS, Leese GP (2009) Decreasing amputation rates in patients with diabetes: A population-based study. Diabet Med 26: 773-777.
- Aulivola B, Hile CN, Hamdan AD, Sheahan MG, Veraldi JR, et al. (2004) Â Major lower extremity amputation outcome of a modern series. Arch Surg 139: 395-399.
Citation: Persiani F, Filippi F, D’Andrea A, Dito R, Ficarelli R, et al. (2019) Complications and Mortality after Major Amputation in Patients with Critical Limb Ischemia: A Single Center Experience. Clin Res Foot Ankle 7:284.
Copyright: © 2019 Persiani F, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Select your language of interest to view the total content in your interested language
Share This Article
Recommended Journals
Open Access Journals
Article Usage
- Total views: 4050
- [From(publication date): 0-2019 - Dec 04, 2025]
- Breakdown by view type
- HTML page views: 3078
- PDF downloads: 972