Effectiveness of Pilates as an Adjunct to Conventional Therapy in Chronic Mechanical Neck Pain: A Randomized Controlled Trial
Received: 01-Feb-2018 / Accepted Date: 23-Feb-2018 / Published Date: 26-Feb-2018 DOI: 10.4172/2165-7025.1000381
Abstract
Background: Neck pain is one of the most common musculoskeletal disorders second to low back pain associated with chronic pain, restricted range of motion and muscular imbalance. Generally, the physiotherapy methods for mechanical neck pain consist of stretching and strengthening the neck muscles, cervical stabilization exercises, cervical mobilization exercises, thoracic thrust manipulation, ischemic compression on trigger points, kinesio-taping method and electrotherapy. The Pilates method is a system of exercise program that aims for body awareness through harmonization of body and mind which has been widely used to enhance physical fitness and rehabilitation in general.
Purpose: The purpose of the study was to find out whether Pilates and conventional therapy can bring better results in treating chronic mechanical neck pain when compared to conventional therapy alone.
Methods: 60 patients were selected randomly with mechanical neck pain. The study included 2 groups, control group and experimental group, the outcomes measures included Numerical rating pain scale (NRPS), Neck flexors endurance test (NFET) Neck disability index (NDI), Cervical range of motion (CROM). Independent “t” test was done for inter group analysis and paired t-test was done for intra group analysis.
Results: Both the groups showed significant difference (P-0.000<0.05) at 12 weeks. The mean difference and paired t-test values of experimental group was greater when compared to control group at the end of 12 weeks.
Conclusion: significant improvement was seen in both the groups in NPRS, NDI, NFET, ROM, but early improvement was noted in experimental group in terms of function when compared to conventional group after 12 weeks of treatment.
Keywords: Mechanical neck pain; Pilates; NPRS; NDI; NFET; IFT
Introduction
Mechanical neck pain is a common problem in the world today and there are epidemiological and statistical studies documenting the high incidence and prevalence of mechanical neck pain, which effects people’s daily function [1]. Nearly 50% of the population suffer from neck pain at least once in their life [2,3], prevalence is high in middle age, with women being affected more than men [3-5] the prevalence of neck pain varies widely between studies, with a mean point prevalence of 7.6% (range 5.9-38.7%) and mean lifetime prevalence of 48.5% (range 12.2-71.0) [6].
The etiology of uncomplicated neck pain is unclear. Most uncomplicated neck pain is insidiously and is generally multifactorial in origin associated with poor posture, anxiety, depression, neck strain, occupational activities and sporting injuries [4,7].
Chronic mechanical neck pain is characterized by pain in cervical region with restricted range of motion and dysfunctional musculature [1]. Reduction of activation of deep cervical flexor muscles (longus coli and longus capitis) is one of the most important factor in mechanical neck pain, superficial neck muscles (sternocleidomastoid and anterior scalene) become over active and painful.
Generally, the physiotherapy methods for mechanical neck pain consist of stretching and strengthening the neck muscles [8] cervical stabilization exercises, cervical mobilization exercises, thoracic thrust manipulation, ischemic compression on trigger points [7-10], kinesiotaping method [2,3] and electrotherapy [11].
Joseph H. Pilates developed the comprehensive program known as the Pilates method in the 1920’s [12]. Pilates is another popular form of mind-body exercises where the focus is on controlled movement, posture and breathing. It is system designed to condition the body as well as improve posture, muscle tone, alignment and provide flexibility by using exercises that stretch and strengthen selective muscles [1,13].
Very few studies have shown the effectiveness of Pilates in treating chronic mechanical neck pain. Pilates exercises were used to strengthen and stabilize the neck muscles. The key is to strength the inner (local) muscles of the neck and ensure the large outer (global) muscles are not being used to support your head [12,14]. However, there are no studies which compared the effectiveness of Pilates combined with conventional therapy alone.
Methods and Study Design
We recruited 60 subjects from Physiotherapy out-patient Department, Nizam’s Institute of Medical Sciences, Hyderabad. Subjects diagnosed with chronic mechanical neck pain by Orthopedic department were included in the study.
Inclusion criteria
Age 18-60 years of both sexes, neck pain and symptoms for more than 6 weeks to 3 months, restricted ROM of neck, mechanical or postural neck pain.
Exclusion criteria
Neck pain radiating to upper limbs (radiculopathy), neurological dysfunctions of neck and upper extremity, history of rheumatoid diseases, open wounds, patients not willing to take part in the study, subjects with conditions and diseases which are contraindicated, ankylosing spondolysis, spondylolysthesis, osteoporosis, osteomyelitis, malignancy, pregnancy and spinal cord syndromes, recent trauma, those who initiated or changed their physical activity regimen in the three months prior to the study, individuals with visual deficiency not corrected by the use of glasses and those who presented diseases of the central nervous system.
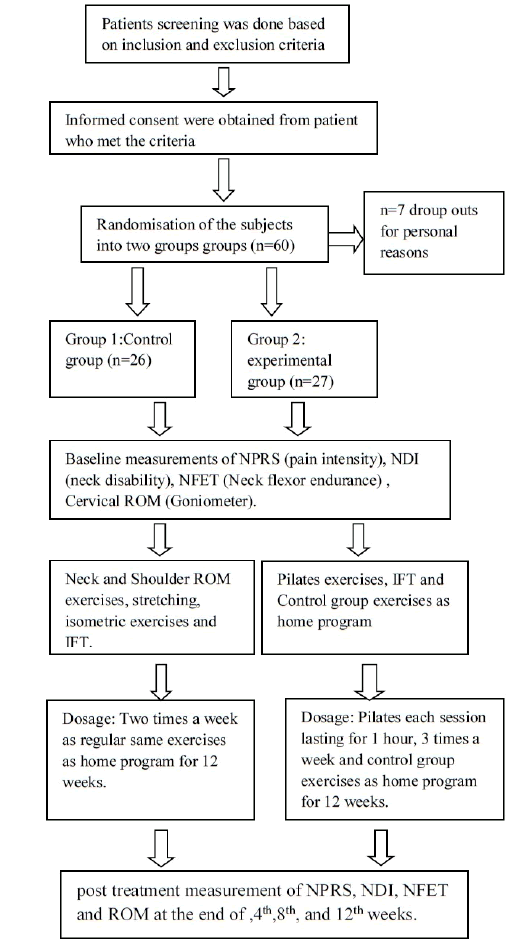
Institution ethical committee approval was taken. The subjects were randomly assigned into 2 groups by the principal investigator using lottery method who met the inclusion and exclusion criteria. The allocations were concealed and the outcome measures were blinded which were taken by the Physiotherapist who was trained to take the outcome measures. Informed consent was obtained from patient who met the criteria, the outcome measurements include Numerical rating pain scale (NRPS), Neck flexors endurance test (NFET), Neck disability index (NDI), cervical range of motion goniometry (CROM). Pretreatment evaluation was done at the first day as baseline measurement, by asking the patient to mark along the line to determine their level of pain on NPRS. The functional disability of each patient was assessed by NDI. The endurance of the deep neck flexors is assessed by NFET and Neck ROM using goniometer. At the end of session (0th day), the subjects were assessed if any increase in pain, if no adverse response were reported. Further sessions were carried out. In group 1 and 2 subjects were taught conventional physiotherapy exercises on 0th day and were advised to perform the exercises at home, based on the dosages mentioned below. 12 contact sessions were given at 48 hours interval for 12 weeks in group 2 and follow up evaluation was done at the end of 4th, 8th, 12th week and documented in two groups.
Group 1
Conventional group subjects received Interferential therapy (IFT) and exercises which included neck active ROM exercises, neck isometric exercises [15,16]. Chin tucks, shoulder ROM and bracing exercises, stretching of the neck extensors and pectorals, moist heat (hot pack) for 10 minutes. Precaution and ergonomic advice [17]. These exercises were given as home program to the subjects.
Dosage: IFT for 8 minutes, exercises 5 sets × 10 repetition with 2 min rest between each set for 12 weeks.
Group 2
Pilates and conventional therapy subjects were individually assessed and taught the 5 key elements of Pilates [13].
Beginner exercises
• Hip twist level 1: active starting position: supine one knee moves away from and then towards midline of the body while maintaining a neutral position of spine. This challenges the rotational control of the lumbar spine.
Consort flow chart of the study
• Double leg stretch level 1: Both the Arms are lowered overhead while maintaining ribcage and pelvic control.
• Double leg stretch level 2: As for level 1 but simultaneously sliding one heel along the mat away from the body.
• One leg stretch level 1: one heel slides along mat extending same leg without allowing the pelvis to anteriorly tilt.
• Clam level 1: starting position: side lying, knees flexed to 90 degrees open the top knee towards the ceiling maintain contact with the medial sides of the feet with hips stacked.
• Shoulder bridge level 1: starting position: crook lying, inhale and during exhalation role the spine up vertebra by vertebra, leading from coccyx and as far as shoulder blades.
• Scissors level 1: starting position: supine, one knee is lifted over the hip (90 degrees angle at the knee and hip) while keeping the pelvis in neutral.
• Arm opening level 1: The uppermost arm is lifted away from the body to open the upper chest and rotate the thoracic and lumbar spine.
• Breast stroke prep level 1: starting position: prone, Shoulder blade glide gently downwards away from the ears while lifting the arms 4-5 cm off the mat.
• Breast stroke prep level 2: As for level 1 with the upper body lengthened off the mat to hover the breastbone 3 cm from the floor while maintaining a neutral lumbo-pelvic position. Keep the back of the neck long. This exercise retrains co-activation of deep and serratus anterior, neck flexors and extensors with upper, lower trapezius [13].
Dosage: Each session lasted one hour and commenced with a tenminute warm up and finished with a 5-10 min cool down. 3 days per week for 12 weeks, IFT for 8 minutes and conventional therapy as home program.
Statistical Design and Data Analysis
Independent T-test
For independent T-test refer Table 1.
| t-test for Equality of Means | T | Df | Sig. (2-tailed) | |
|---|---|---|---|---|
| NFET(sec) 0W | Equal variances assumed | -0.867 | 51 | 0.39 |
| NFET(sec) 4W | Equal variances assumed | -1.221 | 51 | 0.228 |
| NFET(sec) 8W | Equal variances assumed | -4.626 | 51 | 0 |
| NFET(sec) 12W | Equal variances assumed | -6.289 | 51 | 0 |
Table 1: Analysis of, t and P value of NFET with “0”, 4th, 8th, 12th week comparison for control and experimental group.
Paired T-test
For paired T-test refer Tables 2-10.
| Group | Paired Differences Mean | T | Df | Sig. (2-tailed) | |
|---|---|---|---|---|---|
| CON | NPRS 0W-12W | 6.769 | 21.470 | 25 | 0.000 |
| EXP | NPRS 0W-12W | 6.889 | 22.026 | 26 | 0.000 |
Table 2: Analysis of, t and P value of NPRS with “0” week and 12th week comparison for control and experimental group.
| Group | Paired Differences Mean | T | Df | Sig. (2-tailed) | |
|---|---|---|---|---|---|
| CON | NDI (%) 0W-12W | 27.808 | 21.734 | 25 | 0.000 |
| EXP | NDI (%) 0W-12W | 31.333 | 19.789 | 26 | 0.000 |
Table 3: Analysis of, t and P value of NDI with “0” week and 12th week comparison for control and experimental group.
| Group | Paired Differences Mean | T | Df | Sig. (2-tailed) | |
|---|---|---|---|---|---|
| CON | NFET(sec) 0W-12W | -27.462 | -20.395 | 25 | 0.000 |
| EXP | NFET(sec) 0W-12W | -40.704 | -21.888 | 26 | 0.000 |
Table 4: Analysis of, t and P value of NFET with “0” week and 12th week comparison for control and experimental group.
| Group | Paired Differences Mean | T | Df | Sig. (2-tailed) | |
|---|---|---|---|---|---|
| CON | FLX 0-12W | -27.692 | -12.230 | 25 | 0.000 |
| EXP | FLX 0-12W | -30.741 | -14.590 | 26 | 0.000 |
Table 5: Analysis of, t and P value of Flexion with “0” week and 12th week comparison for control and experimental group.
| Group | Paired Differences Mean | T | df | Sig. (2-tailed) | |
|---|---|---|---|---|---|
| CON | EXT 0W 12W | -30.192 | -18.539 | 25 | 0.000 |
| EXP | EXT 0W-12W | -37.037 | -21.348 | 26 | 0.000 |
Table 6: Analysis of, t and P value of Extension with “0” week and 12th week comparison for control and experimental group.
| Group | Paired Differences Mean | T | Df | Sig. (2-tailed) | |
|---|---|---|---|---|---|
| CON | LAT FLX (R) 0W-12W | -17.692 | -8.743 | 25 | 0.000 |
| EXP | LAT FLX (R) 0W-12W | -22.963 | -16.186 | 26 | 0.000 |
Table 7: Analysis of, t and P value of Lateral flexion (R) with “0” week and 12th week comparison for control and experimental group.
| Group | Paired Differences Mean | T | Df | Sig. (2-tailed) | |
|---|---|---|---|---|---|
| CON | LAT FLX 0W-12W L | -16.538 | -8.628 | 25 | 0.000 |
| EXP | LAT FLX 0-12W L | -22.778 | -15.010 | 26 | 0.000 |
Table 8: Analysis of, t and P value of Lateral flexion (L) with “0” week and 12th week comparison for control and experimental group.
| Group | Paired Differences Mean | T | Df | Sig. (2-tailed) | |
|---|---|---|---|---|---|
| CON | ROTATION 0W R-12W R | -16.154 | -10.409 | 25 | 0.000 |
| EXP | ROTATION 0W R-12W R | -18.704 | -11.747 | 26 | 0.000 |
Table 9: Analysis of, t and P value of Rotation (R) with “0” week and 12th week comparison for control and experimental group.
| Group | Paired Differences Mean | T | Df | Sig. (2-tailed) | |
|---|---|---|---|---|---|
| CON | ROTATION 0W-12W L | -14.615 | -8.672 | 25 | 0.000 |
| EXP | ROTATION 0W-12W L | -20.000 | 17.192 | 26 | 0.000 |
Table 10: Analysis of, t and P value of Rotation (L) with “0” week and 12th week comparison for control and experimental group.
Results
Pain
The findings of the present investigation indicated that pain has reduced significantly in both groups evident by the mean value of NPRS. In day 1 mean is 8.12, similarly week 12 mean is 1.35, paired t-value is 21.470, P-value is 0.000<0.05, hence there is a significant decrement in week 12 compared to day 1 NPRS in control group. Similarly, we have in the day 1 experimental mean is 7.56, week 12 mean is 0.67 paired t-value is 22.026, P-value is 0.000<0.05, hence there is a significant decrement in week 12 compared to day 1 NPRS in both the group.
Neck disability
The mean value of control group on day 1 is 38.27 SD is 9.735, similarly week 12 mean is 10.46 and SD is 7.328. Here calculated paired t-value is 21.734 df=25 P-value is 0.000<0.05, similarly we have in the day 1 mean is 36.04 SD is 10.453, similarly week 12 mean is 4.70 and SD is 5.986. Here calculated paired t-value is 19.789, df=26 P-value is 0.000<0.05, hence there is a significant decrement in week 12 compared to day 1 NDI in experimental group than in control group (Figure 1).

Figure 1: Graphical Representation Analysis of, t and P value of NDI with “0” week and 12th week comparison for control and experimental group.
Neck flexor endurance test
The mean value of control group on day 1 is 12.23 SD is 5.233, similarly week 12 mean is 39.69 and SD is 7.509. Here calculated paired t-value is-20.395 df=25 P-value is 0.000<0.05, similarly we have in the day 1 mean is 13.59 SD is 6.141, similarly week 12 mean is 54.30 and SD is 9.269. Here calculated paired t-value is-21.888, df=26 P-value is 0.000<0.05, hence there is a significant better increment in week 12 compared to day 1 NFET in experimental group than in control group (Figure 2).

Figure 2: Graphical Representation of analysis of, t and P value of NFET with “0”, 4th, 8th, 12th week comparison for control and experimental group.
Cervical range of motions
Flexion in control group day 1 mean is 21.92, week 12 mean is 49.62, paired t-value is-12.230, P-value is 0.000<0.05. similarly, we have in the day 1 mean is 22.04, week 12 mean is 52.78. paired t-value is-14.590, P-value is 0.000<0.05, hence there is a better significant increment in week 12 compared to day 1 Flexion in experimental group than in control group.
Extension in control group day 1 mean is 21.54 SD is 6.127, similarly week 12 mean is 51.73. t-value is-18.539, P-value is 0.000<0.05. The day 1 mean is 19.63, week 12 mean is 56.67. paired t-value is-21.348, P-value is 0.000<0.05, hence there is a better significant increment in week 12 compared to day 1 extension in experimental group. Cervical rotations right control group day 1 mean 26.15, week 12 mean is 42.31. paired t-value is-10.409, P-value is 0.000<0.05, similarly day 1 mean is 25.74, week 12 mean is 44.44. paired t-value is-11.747, P-value is 0.000<0.05, hence there is a significant increment in week 12 compared to day 1 Rotation (R) in both groups but better significant in experimental group. rotation (L) day 1 mean 27.50, week 12 mean is 42.12 and paired t-value is-8.672 P-value is 0.000<0.05, similarly we have in the day 1 mean is 24.44, week 12 mean is 44.44. paired t-value is-17.192-, P-value is 0.000<0.05, hence there is a significant increment in week 12 compared to day 1 in both the group but better significant increment is seen in Rotation (L) in exp group. Lateral flexion control group day 1 mean 24.42, week 12 mean is 42.12. paired t-value is-8.743, P-value is 0.000<0.05, day 1 mean is 21.11, week 12 mean is 44.07. paired t-value is-16.186, P-value is 0.000<0.05, hence there was significant increment in week 12 compared to day 1 Lateral flexion (R) in both the groups but better significant in exp group. Lateral flexion (L) day 1 mean 25.58, week 12 mean is 42.12. paired t-value is-8.628, P-value is 0.000<0.05, day 1 mean is 21.30, week 12 mean is 44.07. paired t-value is-15.010, P-value is 0.000<0.05, hence there was significant increment in week 12 compared to day 1 Lateral flexion (L) in both the groups but better significant increment was seen in experimental group.
Discussion
The study describes to compare the effectiveness of 12 weeks Pilates and conventional physical therapy treatment used adjunct to conventional therapy alone on individuals with chronic mechanical neck pain in improving pain, Range of motion, muscle performance and functional disabilities of neck.
According to the data collected the percentage distribution of gender of. Majority i.e., 56.6% of them were female, while 43.4% of them were males.
Pain is associated with altered muscle recruitment patterns; high level of muscle contraction and tone shortens muscles and creates exaggerated muscle imbalances and thus more pain [18]. The Pilates program in this study focused on improving systematic balances rather than specific (cervical or thoracic) regions, which emphasizes core stability and spinal separation. Furthermore, the additional benefits of Pilates exercises include decreased hypertension in shortened and weakened muscles during exercise [19]; improved breathing methods (diaphragmatic and rib breathing) that improve core stability; and increased awareness of postural misalignments. The results of this study indicate that Pilates training results in whole-body muscle retraining, which strengthens the deep neck muscles and thus reduce neck pain. However, the effect of IFT would also result in being more tolerable by decreasing the pain perception.
Neck disability
It is suggested that as the disability score aims to assess different aspects of clinical symptoms of neck pain (which consists of pain intensity, daily activities, work and social activities) the improvement in disability score might be due to the combined effects of reduction in neck pain, improvement in neck muscle strength and endurance and to certain extent improvement in activities of daily living [16,20].
Neck flexor endurance test
It might be suggested that the gain in the strength in these subjects was likely a result of increased confidence. It might be explained that the strength increase in the experimental group was probably due to biological variation and learning effect due to repeated testing. Similarly, it could be suggested that an improvement in cognitive perception of pain might contribute to the improvement of muscle strength in patients with chronic neck pain [21,22].
Cervical range of motion
The pilates technique focuses on the “core musculature” it starts by stabilizing the core musculature and then proceeds through a controlled range of motion. However the effect of IFT would also result in cervical ROM being more tolerable by decreasing the pain perception, which would allow the muscles to be strengthen to a greater degree resulting in a greater amount of flexion, extension, rotation and lateral flexion. Extension of the head and neck is the primary function of the posterior cervical muscles so treatment of this muscle group would have a positive effect on extension with regard to increasing the extension range of motion. This assertion proved correct and results were positive. Flexion, Extension, lateral flexion and rotation shows that there was better significance difference in experimental group than the control group [23-27].
Conclusion
From the results obtained, it can be concluded that significant improvement is seen in both the groups but based on the statistical mean early improvement was noted in experimental group, so Pilates may be helpful in faster recovery in terms of function in treating chronic mechanical neck pain when compared to conventional therapy alone after 12 weeks of treatment.
Overall, it was shown that Pilates as an adjunct to conventional therapy is more effective when compared with conventional therapy alone in reducing pain, cervical range of motion, muscular imbalance and disability in subjects with chronic mechanical neck pain.
However, further studies are needed using large sample size.
Limitations
• Limited sample size.
• Unadvisable activities (lifting heaving objects) carried out at home inspite of ergonomic advice was not monitored.
Scope for Further Study
• Better results can be drawn if the study was conducted with large sample size.
• Different age groups can be included and studied separately to draw significant results.
More quantitative or objective measures can be used to measure the outcomes in mechanical neck pain.
References
- Carine BS (2009) Relative effectiveness of using Pilates exercises to obtain scapular stabilization as adjunct to cervical manipulation in the treatment of chronic mechanical neck pain.
- Kilinc HE, Harput G, Baltaci G (2015) Additional effects of kinesiotaping to mobilization techniques in chronic mechanical neck pain. Turk J Physiotherapy Rehabilitation 26: 107-113
- Cote P, Cassidy JD, Carroll L (1998) The Saskatchewan Health and Back Pain Survey. The prevalence of neck pain and related disability in Saskatchewan adults. Spine 27: 1689-1698.
- Makela M, Markku H, Kai S, Olli I, Paul K, et al. (1991) Prevalence, determinants and consequences of chronic neck pain in Finland. American Journal Epidemiology 134: 1356-1367.
- Fejer R, Kyvik KO, Hartvigsen J (2006) The prevalence of neck pain in the world population: a systemic critical review of the literature. Euro Spine J 15: 834-848.
- Damgaard P, Bartels EM, Inge R, Christensen R, Juul-Kristensen B (2013) Evidence of physiotherapy interventions for patients with chronic neck pain: A systematic review of randomized controlled trails. ISRN Pain, Article ID 567175, p: 23.
- Ylinenet J, Takala EP, Nykänen M, Häkkinen A, Mälkiä E, et al. (2003) Active neck muscle training in the treatment of chronic neck pain in women: A randomized controlled trail. JAMA 289: 2509-2516.
- Childs J, Cleland JA, Elliott JM, Teyhen DS, Wainner RS, et al. (2008) Neck pain: Clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedicsection of the American physical therapy association. J Ortho Sports Phys Ther 38: 1-34.
- Vemon H, Humphreys K, Hagino C (2007) Chronic mechanical neck pain in adults treated by manual therapy: A systemic review of changes score in randomized controlled trials of a single session. Journal of Manual and Manipulative Therapy 16: 215-217.
- Jorge P, Armijo Olivo S, Magee DJ, Gross DP (2010) Effectiveness of interferential therapy in the management of musculoskeletal pain: A systemic review and meta-analysis a research report. Phys Ther 90: 1219-1238.
- Megan MH, Eric Hegedus J (2008) Multimodal management of mechanical neck pain using a treatment ased classification system. J Man & Manupla Ther 16: 217-224.
- Mallin G, Murphy S (2013) Effectiveness of 6 weeks Pilates programme on outcome measures in a population of chronic neck pain patients: A pilot study. J Bodyw Mov Ther 17: 376-384.
- Susan S, Stilp S, Akuthota V (2008) Yoga and pilates in the management of low back pain. Curr Rev Musculoskelet Med 1: 39-47.
- Petric PK, Ylinen JJ, Mälkiä EA, Kautiainen H, Häkkinen AH (2006) Isometric strength of the cervical flexor, extensor and rotator muscles in 220 health females aged 20 to 59 years. J Orthop Sports Phys Ther 36: 495-502.
- Griffths C, Dziedzic K, Waterfield J, Sim J (2009) Effectiveness of specific neck stabilization exercises or a general neck exercises program for chronic neck disorder: A randomized controlled trail. J Rheumatol 36: 390-397.
- Pool JJ, Ostelo RW, Hoving JL, Bouter LM, de Vet HC (2007) Minimal clinically important change of the Neck Disability Index and the Numerical Rating scale for patients with Neck pain. Spine 32: 3047-3051.
- Shirley S (2001) Diagnosis and Treatment of Movement Impairment Syndromes. Mosby, St. Louis.
- Janda V (1994) Muscles and Motor Control in Cervicogenic Disorders: Assessment and Management. Churchill Livingstone, New York, USA.
- Richard L, Gajdosik RW (1987) Clinical measurement of range of motion: Review of goniometry emphasizing reliability and validity. Phys Ther 67: 1867-1872.
- Farrar T, Young JP, LaMoreaux L, Werth JL, Poole RM (2001) Clinical importance of change in chronic pain intensity measured on an 11-point numerical pain rating scale. University of Pennsylvania School of Medicine 94: 149-158.
- Lucas H, O'Leary EF, Niere KR, Green S, Buchbinder R (2002) Validity of the neck disability index, Northwick park neck pain questionnaire, and problem elicitation technique for measuring disability associated with whiplash-associated disorders. Pain 102: 273-281.
- Cazotti LA (2015) AB1229-HPR effectiveness of the Pilates method in the treatment of chronic mechanical-postural neck pain. Annals of Rheumatic Diseases. Eular Journal, pp: 1345-1346.
- Paolo P, de Lima E, Sá Resende F, Banchelli F, Burioli A, et al. (2016) Effectiveness of global postural re-education in patients with chronic nonspecific neck pain: randomized controlled trail. Phys Ther 96: 1408-1416.
- Kevin DH, Heer DM, Roy TC, Santos DM, Whitman JM, et al. (2005) Reliability of a measurement of neck flexor muscle endurance. Phys Ther 85: 1349-1355.
- Olson LE, Millar AL, Dunker J, Hicks J, Glanz D (2006) Reliability of a clinical test for deep cervical flexor endurance. J Manipulative Physiol Ther 29: 134-138.
- Lee SM, Lee CH, O'Sullivan D, Jung JH, Park JJ (2006) Clinical effectiveness of Pilates treatment for forward head posture. Journal of Physical Therapy Science 28: 2009-2013.
Citation: Nandita E, Dowle P, Asif Hussain KS (2018) Effectiveness of Pilates as an Adjunct to Conventional Therapy in Chronic Mechanical Neck Pain: A Randomized Controlled Trial. J Nov Physiother 8: 381. DOI: 10.4172/2165-7025.1000381
Copyright: © 2018 Nandita E, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Select your language of interest to view the total content in your interested language
Share This Article
Recommended Journals
Open Access Journals
Article Tools
Article Usage
- Total views: 7301
- [From(publication date): 0-2018 - Dec 20, 2025]
- Breakdown by view type
- HTML page views: 6204
- PDF downloads: 1097