Thesis Open Access
Knowledge, Attitude, and Practice of Voluntary Blood Donation and Associated Factors among Health Care Providers in Addis Ababa health Facilities, Ethiopia
Destaw Bantayehu*Debre Markos University and Gamby College of Medical Sciences, Joint MPH Program, EthiopiaSciences, Lahore, Pakistan
- *Corresponding Author:
- Destaw Bantayehu
Debre Markos University and Gamby
College of Medical Sciences
Joint MPH Program, Ethiopia
Tel: +251 (0) 911767379
Fax: +251 (0) 911767379
E-mail: destwab1@yahoo.com
Received date: June 26, 2015; Accepted date: July 30, 2015; Published date: August 08, 2015
Citation:Bantayehu D (2015) Knowledge, Attitude, and Practice of Voluntary Blood Donation and Associated Factors among Health Care Providers in Addis Ababa health Facilities, Ethiopia. Occup Med Health Aff 3:209. doi: 10.4172/2329-6879.1000209
Copyright: ©2015 Bantayehu D. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Visit for more related articles at Occupational Medicine & Health Affairs
Abstract
Background: The discovery of blood circulation in 1628 has made an important mile stone in the history of transfusion medicine. Although the first successful blood transfusion occurred in 1818, scientists had put quite a lot of effort earlier than this period. Despite the fact that blood transfusion service has about 200 years of history, there is still a significance shortage of blood and blood products particularly in the developing world. In 2010 the annual blood demand of Ethiopia was estimated to be about 100,000 units per year, yet 44 686 units of blood were collected by the Ethiopian Red Cross Society in the same year. Of which, only 22% were collected from voluntary non remunerated sources. Health care providers could also be a potential source of voluntary blood donation if we encourage them. Objective: to assess the level of knowledge, attitude and practice (KAP) of health care providers in Addis Ababa health facilities towards voluntary blood donation and identify the possible determinants of blood donation practice
Methods: Facility based cross sectional analytic study was used. To select the participants and determine the sample size, multistage sampling technique with a design effect of two was employed; hence the total sample size became 808 using single population proportion formula. Structured questionnaire which is adapted from other published journals were used. The data collected were cleaned, coded and entered to computer. SPSS version 20 was used for data analysis and management. 95% confidence level with 5% margin of error was tolerated.
Result: The level of knowledge determined in this study was found to be good for 72.7% of the respondents. Availability of blood transfusion services within the facility is one of the factors which affect the level knowledge of the participants. 81.7% of respondents have a positive attitude towards blood donation and being male increases the odds of favorable attitude. 32.6% has ever donated blood at least once in their life time yet only less than half of the overall donors are donated blood based on sense of voluntarism.
Conclusions and recommendations: although there was a good level of favorable attitude observed in this study, the level of knowledge as well as the practice of blood donation is found to be something that needs attention. Perhaps to create more awareness and sensitization among health care workers to wards voluntary blood donation would be worthy to improve them.
Keywords
Health; Blood donation; Transfusion
Acronyms and Abbreviations
AAU: Addis Ababa University; ART: Antiretroviral Therapy; BD: Blood Donation; CDC: Center for Disease control and prevention; EPI: Expanded program of Immunization; ERCS: Ethiopian Red Cross Society; ETB: Ethiopian Birr; MOH: Ministry of Health; HBV: Hepatitis B virus; HIV: Human Immunodeficiency Virus; HSDP: Health Sector Development Program; IFRC: International Federation of Red Cross and Red Crescent Societies; KAP: Knowledge, Attitude and Practice; MCH: Maternal and Child Health; MOH: Ministry Of Health; NR: No Response; OR: Operation Room; SPSS: Statistical Package for the Social Sciences; TTI: Transfusion-transmissible infections; VBD: Voluntary blood donation; WHO: World Health Organization
Introduction
Background
After the discovery of circulation of blood in 1628 by British Physician, William Harvey, the field of transfusion medicine has made an important progress since then. Shortly afterwards the first known blood transfusion attempt was done. However, the first recorded successful dog to dog blood transfusion occurred 37 years later by English physician Richard Lower In 1665. In 1818 a patient of postpartum hemorrhage received the first human blood successfully by the British obstetrician [1].
About 108 million blood donations were collected globally in 2013. Nevertheless almost half of these are collected in high-income countries, home to only 18% of the world’s population. The remaining 82% of the world’s population contributed for half of the overall blood collections across the globe [2].
The demand of blood and its components increased dramatically during the Second World War and immediate post war period in the United States of America. As a result of this rapid establishment and growth of blood banks, transfusion services, and other related support services were noticed across the country [3].
Although there has been an increase of almost 8 million blood donations from voluntary unpaid donors from 2004 to 2011, there are chronic shortages of safe blood and blood products in many countries, so blood transfusion is not available for many of the world’s most vulnerable populations [4].
Although, ideally blood transfusion is a safe process, there are a number of risks associated with transfusion such as; viral, bacterial and parasitic infection on recipient. At times when individuals lost large volume of blood due to serious accidents, obstetric hemorrhages or any other causes of anemia due to medical or surgical conditions, blood transfusion could be lifesaving procedures. Therefore, ensuring the availability of safe blood at all times would have greater value for saving life through transfusion for those who needed it most [5,6].
Blood services in Ethiopia have been mainly provided by the Ethiopian Red Cross Society (ERCS) since 1969. Blood bank and transfusion services include collection, processing, storage and provide human blood intended for transfusion. Blood from the ERCS suffices only for the needs of 52% of the national hospitals in the country [2,7,8].
Although the Ethiopian Red Cross Society has been the one who took the lead and initiative in developing blood banking services in the country, blood transfusion services in Ethiopia are still rely on family and replacement donors [7].
Adequate and safe blood supply has remained a challenge in developing countries including Ethiopia. There is a high dependency on family replacement and remunerated blood donors in our environment which carries an attendant increased risk of transfusion transmissible infection.
In Ethiopia, family replacement blood donation accounts for 70% of the overall blood donations across the country. Furthermore, because of the high prevalence of some infectious disease; such as hepatitis B, C and HIV, selection of donors are often not easy [7,9].
Statement of the problem
Blood transfusion saves lives and improves health nevertheless access to equitable and safe blood is still challenging for many of those who need it most. Despite the fact that there is an increase of blood donations from voluntary unpaid donors in recent years (according to The International Federation of Red Cross and Red Crescent Societies (IFRC) 2012 report, 8 million more donations were recorded in 2011 when compared to 2004) , there is shortage of active blood donors to meet the increased demands of blood. In addition to limited supply, the safety especially with regard to the risk of transfusion transmissible infection is also an issue and one of concerns especially in the developing countries [4,6,8].
Even though blood has an important value of one’s own society and the health system, unless we ensure the safety of these products, it may be complicated by infectious conditions and immunological disorders which might bring serious complications or even could be fatal [10].
World Health Organization’s (WHO) 2014 report indicated that a total of about 10 000 blood centers exist globally. 83 million donations in 168 countries reported. In the low- and middle-income countries, the median annual donation per center was 3100 compared to 15 000 in the high income countries. This shows that there is a significant access difference of blood amongst the low- and high-income countries [2].
Even though the prevalence of adequate knowledge towards blood donation is estimated to be 60% in developing countries, the blood donation rate in low income countries is far less than that of the middle and high income countries; which is 3.9 donation in low income countries per 1000 population compared to 36.8 and 11.7 donations per 1000 population in high-income and middle income countries respectively [2,11].
The prevalence of transfusion-transmissible infections (TTI) in blood donations ranges from 0.002% in high-income countries to 0.85% in low income countries for HIV. Hepatitis B Virus (HBV) infections prevalence among blood donations reaches as high as 6% in low income countries. Therefore transmission of Transfusion-Transmissible Infections (TTI) is preventable by establishing an adequate supply of safe blood through voluntary blood donation practices [12].
Anemia, one of the conditions which require blood transfusion in its severe form, prevalence among children and child bearing women in Ethiopia is 44 % and 17% respectively. Of which 3% of children and 1 % of child bearing women have severe anemia [13].
The Ministry of Health (MOH) of Ethiopia recognizes the insufficiency of adequate and safe blood supply across the nation. Since the beginning of the fourth Ethiopian Health Sector Development Program (HSDP IV) , the construction of 21 blood banks are ongoing. Shortage of adequate and safe blood supply was one of the challenges and implementation gaps in HSDP III and hence it was recommended to fasten the completion and functionality of the newly constructed blood banks in HSDP IV [11].
Access to safe and adequate blood supply remains a challenge in Ethiopia. 44 686 units of blood were collected by the Ethiopian Red Cross Society in 2010 compared to the estimated annual demand of 100 000 units of blood. On the same year, according to the CDC 2011 report, Neighboring Kenya, half the population size of Ethiopia, managed to collect 135, 565 units of blood. Similarly the blood donation rate of Ethiopia was remained at 0.5 donations per 1000 population as compared to 18.2 in South Africa. Moreover, Addis Ababa city Administration accounts for 70% of the collection and utilization of those bloods. Only 30% of these units go to the remaining large segment of the population [8,14].
In 2010 WHO estimates the blood demand of the country is estimated to be 100 000 units per year.Due to lack of adequate regular volunteer non remunerated blood donors, The Ethiopian Red Cross Society National Blood Bank Service cannot achieve this demand at present [2,7].
Taking into account the big demand for safe blood and blood products across the nation and understanding the role of blood centers in the prevention of transfusion transmissible diseases, the Ethiopian Ministry of Health (MOH) therefore developed national blood transfusion services strategy in 2005 [5].
Voluntary unpaid donors are considered to be the safest compared to family replacement, remunerated or paid donors since this group of donors give blood on a regular basis and hence blood born infections are lowest among voluntary donors. Despite the fact that voluntary blood donation has this very important added value, unfortunately Ethiopia had managed to collect only 23.5% of the overall blood collections from voluntary blood donors source in 2010 while neighboring Kenya and Uganda secured 100% of their blood and blood products from voluntary unpaid blood donors in the same year [6,13].
Literature review
Overview and magnitude of knowledge attitude and practice of blood : WHO recognized the existence of a significance dependency on family/relative replacement and remunerated donors in developing countries in the Melbourne declaration and advocates the establishment of national blood transfusion services that functions on the basis of voluntary, non-remunerable blood donation by member states [15].
Low levels of knowledge and practice were observed in a number of published studies across the developing world. A study conducted among Health Science students in South India revealed that only 42.7% of the respondents have acquired good knowledge on blood donation similarly larger proportion of respondents (62%) never donated blood in their entire life. However, an encouraging figure (87.3%) was observed as having a positive attitude towards blood donation with in the same study [16]. A similar study, to determine the association between knowledge level and other associated factors like gender, among Indian Medical students revealed the prevalence of blood donation rate of among students were only 13.1%. Although this is far less compared to the estimated 60% in developing countries, the findings are much closer to the study conducted by Pravin and Keerti [11,16].
In another but similar study conducted on physicians in Nigerian tertiary health facility indicates that, physicians have good knowledge of voluntary blood donation and a positive attitude towards blood donation [10]. According to this study, 41.4% of physicians had donated blood in the past which is a bit higher compared to the previous studies in India. 8.6% of respondents practiced blood donation more than three times a year. Among the overall donors, majority (53.4%) donated based on sense of voluntarism [10].
Another study on knowledge, attitude and practice about blood donation in the urban population of Yazd, Iran, shows that the level of knowledge of the population under study about services of blood transfusion centers and uses of blood and blood products was relatively good, however despite this fact, only a small percentage of respondents donated blood [17]. Study by Mullah et al. assessing the knowledge and perception of healthcare support staffs of a tertiary healthcare facility in Gujarat revealed a poor knowledge where 51.6 5 of respondents have acceptable knowledge and 91% of them perceive blood donation as unsafe [18].
A similar study carried out in Thailand indicates that 89% of respondents never donated blood in their entire life. This result is in agreement with a study conducted among youngsters in Sikkim by Shenga which indicates 87.3% had never donated blood. Similarly 42.7% the overall respondents acquired a good knowledge level which is far less compared with the studies conducted Among Addis Ababa university students and Nigerian health care workers [19,20].
Factors affecting knowledge attitude and practice of blood donation
As Amit and Aseem explained in their study, the awareness of blood donation was found to be increased when the level of education is getting higher. This finding was also supported with a study conducted on Addis Ababa University (AAU) Medical students which revealed as knowledge is statistically associated with year of study but in contrary with the findings of Benedict N and Usimenahon A, where they found out that educational status and staff category did not have significant association with the practice of blood donation. This is also supported by Salaudeen and Odeh with their study on Knowledge and behavior in which they observed literacy level does not affect the knowledge of the respondents. On the other hand those three studies are in agreement when it comes to the reason for non-donation. All of them found that lack of awareness is the main cause of non-donation by non-donors [10,21-23].
On the other hand, contrary to the above findings, a study performed by Manikandan, Srikumar and P Ruvanthik among 400 health care professionals in India found that the reasons for non-donations were no one has ever asked to donate blood rather than luck of awareness [24].
A study conducted on knowledge, attitude, and practice (KAP) of voluntary blood donation among medical students in India concluded that medical students are well aware regarding blood donation and have positive perception Nevertheless, very few proportion practiced blood donation. Moreover being male is significantly associated with blood donation which is in agreement with the findings of a study conducted among Medical students in AA university, Nigerian physicians and health care workers where males are highly likely to donate blood than females. [10,16,24]
In contrast to this, a study conducted on Knowledge, Attitude, and Practice of Voluntary Blood Donation among Healthcare Workers at the University of Benin Teaching Hospital revealed that there is a significant association between blood donation practice with category of staff and level of education [10]. Among the respondents only 22.1% of them have donated blood in the past, out of which 52.8% were as family replacement and 41.7% voluntary despite the fact that all study participants are within the age range of potential donors [10,18].
Purushottam observed a statistically significant association between knowledge of blood donation and students from different specialties on their study over KAP of blood donations among Medical students in India, this finding is in agreement with a study conducted in AA university where year of study and department is found to be a factor of knowledge [24,25].
Socio demographic status such as age and ethnicity did not show significant relationship with knowledge about voluntary blood donation according to a study carried out by Salaudeen and Odeh on Knowledge and behavior towards voluntary blood donation [23]. Similarly knowledge level and gender do not show any statistical association in a study conducted among medical students in south Indi. In fact this find was also supported by a study carried out in Chile [26]. Another research done on nursing students by Pravin N Yerpude1, Keerti S Jogdand in India revealed that majority 87.23% of students never donated blood which is significantly low compared to other studies. In this study the main reasons stated by non –donors for not donating blood were (29.27%) students never thought about donating blood and due to fear of sickness or complications which contradicts the findings of the above studies [5].
Justification of the study
Since blood transfusion is one of the lifesaving medical procedures, and Ethiopia’s current blood supply is far less compared to the demand, Ensuring adequate blood supply would be vital for the health care system. This can only be achieved by securing sustainable voluntary blood donors with in the community.
Healthcare institutions and its workers, since they are expected to be more aware than the general population, should take the lead to create awareness on blood donations among the population. They also constitute a potential pool of eligible voluntary donors when it comes to voluntary blood donations. Therefore determining the level of knowledge, attitude and practice among the health care providers would be helpful to identify the gaps and implement appropriate strategies with in the institution.
Literatures on knowledge, attitude and practice of voluntary blood donations are hardly available in our settings. Furthermore, it is almost impossible to find a published literature particularly on health care workers in Ethiopia. Therefore, this research would help to fill the existing gaps in this regard
Significance of the study
The results of this study will be beneficial for health personnel, planners, policy makers, Non-Governmental Organizations and others who are engaged in Blood donation activities. Hence, the findings of this research will be disseminated to the relevant bodies, actors and others who are involved in improving the Knowledge, Attitude and Practice of voluntary blood donation.
Voluntary unpaid blood donors are the safest group of blood donors and they could be the source of sustainable national blood supplies sufficient for the countries blood demand. Having the findings of this study, policy makers can use of it to determine appropriate strategies to enhance voluntary blood donation practice among Health care workers (HCW) s.
HCWs, by virtue of their training and medical practices, are expected to be highly informed on the processes of donor blood procurement and the challenges of supply as well as the potential hazards of transfusion. The end result of this study would identify the possible gaps as well as potential area of intervention to improve KAP of health care providers.
Objectives of the study
General objective: To assess the knowledge, attitude and practice of health care providers and associated factors towards blood donation in Addis Ababa health facilities.
Specific objectives: To determine the knowledge of health care workers towards blood donation
To find out the attitude of health care workers towards blood donation.
To assess the practice of health care workers towards blood donation.
To identify the factors affecting the knowledge, attitude and practice of blood donation
among health care providers (Figure 1).
Figure 1: Conceptual framework which indicates the link between the different factors.
Methods
Study design
Facility based cross-sectional study design were employed to conduct this survey.
Study area
The Study was conducted in both government and private health facilities in Addis Ababa city administration in October/November 2014. Addis Ababa, home of an estimated of 3,167,036 people (according to the 2007 national censes), is located in the central part of the country.
According to Addis Ababa health bureau health institution data base the total number of health facilities in Addis Ababa city administration were 775. Of which 683 were either medium or higher clinics located across the city. Kolfe Keranio sub city has the largest concentration of clinics (105) while Gulele sub city accounted for 5.3% of the overall distribution [27,28].
In 2012 a total of forty nine hospitals were functional in the city about 33 of them being private owned and 3 of them were charity based facilities in which services are provided either for free or based on cost recovery. The remaining 13 hospitals were public facilities located in different sub cities of the capital. Bole sub city got the largest concentration of private hospitals (about 27%) followed by Arada subcity where 5 (15%) of the private owned hospitals located [29].
A total of 43 health centers were available across the city, majority of which were governmental institution and only 4 health centers were belong to private owner ship. Moreover 42 health posts were operational in 2014 [28,29].
Among the overall nurses and physicians working in the country in 2013, Addis Ababa city administration accounts for being a home of 45% and 28% physicians and nurses respectively. In 2012 there were a total of 3368 health professionals in Addis Ababa health facilities [28] (Table 1).
| Sub city | Yeka | Kolfe | Bole | Addis | Arada | Lideta | Gulele | Akaki | Kirkos | Nifas | Total | |
| keraniyo | Ketema | Kaliti | Silk | |||||||||
| Lafto | ||||||||||||
| Privately owned | Clinics | 85 | 105 | 61 | 68 | 69 | 41 | 36 | 43 | 91 | 84 | 683 |
| Hospitals | 4 | 1 | 9 | 3 | 5 | 3 | - | 2 | 5 | 1 | 33 | |
| Health Centre |
- | - | 2 | 1 | 1 | - | - | - | - | - | 4 | |
| Public Facilities | Hospitals | 1 | 4 | 1 | 3 | 1 | 3 | 13 | ||||
| Health Centre |
3 | 4 | 4 | 1 | 3 | 3 | 8 | 3 | 3 | 7 | 39 | |
| Non- Profit facilities |
Hospitals | - | - | 1 | - | 1 | - | 1 | - | - | - | 3 |
Table 1: Distribution of different levels of health facilities in Addis Ababa city in 2012.
Source population
All health care workers in Addis Ababa city administration working in the government as well as private or non-profit health institutions.
Study population
The study population were those health care workers (individuals) who were employees of selected institutions where the sample population was drawn.
Sample size
Sample size was determined based on the following assumptions; confidence level was fixed as (1- a) to be 95%, and a p value of <0.05 to be significant. The extent of blood donation practice among the study participants was taken as 50% since there is no published study which shows the prevalence of Knowledge or practice towards blood donation,
Where Z=standard score at 95% CI which is 1.96
P=the prevalence of knowledge, Attitude and practice of blood donation among health care workers. However, eventually the blood donation practice was the most important dependent variable to be determined; hence P for practice was set at 50% since there is no local study on blood donation practice among health care workers available.
d=the margin of error to be tolerated, 0.05
Then 
n=384, plus 5% for non-response rate =404
Since multistage sampling technique was employed, a design effect of 2 was included; hence the total sample size needed to conduct the research was 808.
Therefore a total of 808 eligible health care workers were selected for comprehensive self-administered questioners using a structured pre-tested tool.
Sampling procedure
Multi stage sampling technique was executed. The primary procedure was to select the sub cities in which further selection of the health facilities undergo. Therefore, three sub cities namely Kirokos, Arada and Bole were selected using lottery method among the existing ten administration sub cities of Addis Ababa. Subsequently all health facilities within those selected sub cities were stratified as clinics, health centres, hospitals and non-profit health institution for further selection of the health facilities where the data collection would take place. Based on the average number of health care workers estimated to present at each facility level, it was required to have 6 hospitals, 3 health centres, and 9 clinics in order to fully suffice the sample size comfortably.
Selection of health facilities:
After listing down all the hospitals in each selected sub cities, a simple random lottery method was used to choose the last two hospitals in each sub cities. In this way three public hospitals, two private hospitals and one non-profit hospital were selected. With the same manner, three health centres, all of them being public facilities, were selected from the three sub cities. Similar procedure applied for the selection of the clinics too.
Selection of the study subjects
Data collectors were given the required amount of samples that need to be collected for each selected facility. After obtaining lists of employees of those selected health facilities from the respective institution, data collectors use a systemic random sampling technique to choose the participants of the study. When the nth individuals were not voluntary to participate on the study, the next individual were replaced (Figure 2).
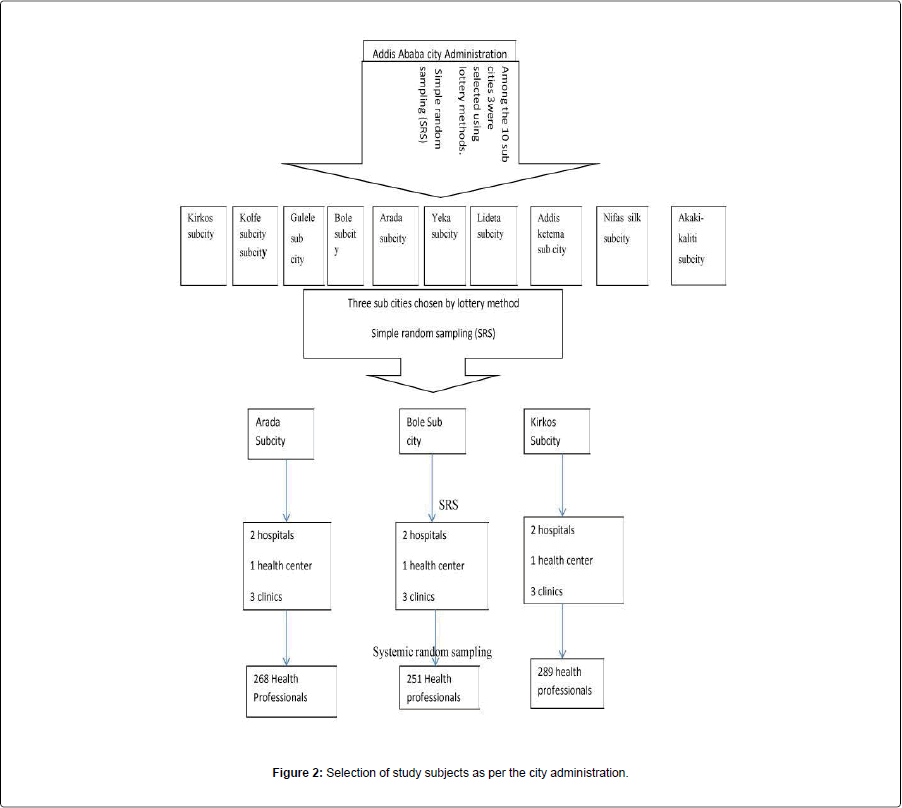
Figure 2: Selection of study subjects as per the city administration.
Inclusion and exclusion criteria
Inclusion criteria: All health care workers, who were employed in Addis Ababa health facilities during the study period and who were voluntary to participate in the study population, were included.
Exclusion criteria: Those health care workers who were seriously sick during data collections were excluded from the study.
Variables
Dependent variables: Knowledge, attitude and practice of health care workers towards blood donation.
Independent variables: Socio demographic profiles such as; age, sex, marital status, religion, profession, access to information, department, availability of blood donation service with in the facility, motivation by previous volunteers, organization of blood donation campaign, and exposure to mass media. Distance (in kilometres) of the nearest blood donation center, history of previous HIV test.
Operational definitions
Safe blood: Means blood that is free from transfusion transmissible diseases, drugs, alcohol, chemical substances, or other extraneous factors that might cause harm or danger to the recipient.
Health care professional: Is an individual that provides preventive, curative, promotional or rehabilitative health care services for individuals or community.
Health Institutions: Government, private or NGO supported health facilities which provide curative, preventive, promotional and/ or rehabilitative services to the population
Knowledge: Nine major questions which had 17 right answers were provided to each participants (since there were more than one correct answer in each of the questions), those who have answered above the 50th percentile of the score were considered to be having adequate knowledge. The rest were categorized as insufficient knowledge.
Attitude: There were five questions in this section to be answered. Respondents who answered at least three questions correctly were considered as favorable attitude. Those individuals who gave a correct answer of two or less were identified as unfavorable attitude towards blood donation.
Practice: Denotes when individuals experienced blood donation activity at least once in their life time.
Voluntary donors: those individuals who donate blood without receiving neither payment nor a replacement for family or friends but only for internally generated sense of altruism or community responsibility.
Remunerated donors: Are individuals who give blood in return for money or other form of payment.
Family replacement donors: These are donors of blood to substitute or replace blood in need of their relatives or friends.
Data collection procedures and quality assurance
A standard questionnaire which was obtained from other published journal articles was used for this study. However, to meet the objectives of the study as well as taking into the local context, the questionnaire was adapted and modified slightly in line with the local context. It was designed in the way that to collect information about all the relevant variables. The data collection instrument had four parts; the first part involved question used to gather information about socio-demographic characteristics, the second part was committed to explore knowledge of health care workers about blood donation, the third part in purposeful to know the attitude of health workers toward blood donation and the final part is focused on the health workers practice to blood donation.
Data collectors were recruited among medical staffs who completed a minimum of diploma level. Supervisors were public health officer graduates and selected based on their experience in supervision and data collection.
Training was given for one day by the principal investigators to data collectors and supervisors prior to data collection. The training was focused on understanding the meaning of each question, obtaining consent, keeping confidentiality of the information they gathered and quality of data collection. Emphasis was given on the significance and appropriate meanings of each question as well as how to explain for the participants in understandable manner if required.
Questionnaires were carefully designed and pre tested with individuals equivalent to 5% of the calculated sample size among Medicines Sans Frontiers health workers who are working on clinical settings. Questionnaires were amended after the pretested results revealed lack of clarity for certain responses. For example, it was discovered that respondents tend to understand the English version of the questionnaires than the Amharic. Therefore findings and experiences obtained from the pre-testing were utilized in modifying and reshaping the research methods, the time needed and the data collection tools (Annexure 1).
Supervision and quality control
Supervision was conducted by two supervisors and the principal investigator as much as possible. Filled questionnaires were reviewed randomly by supervisors and the PIs to check for completeness.
Data management and analysis
The data collected were cleaned, coded and entered to computer using SPSS version 20 for analysis and interpretation. Descriptive and analytic (bivariate and multivariate) logistic regressions analysis was implemented to explore and determine the relationship of predictors on outcome variables. Multiple logistic regression analysis was used to control confounders.
In this study, a p value of <0.05 was considered as statistically significant with 95% confidence level and 5% margin of error. Chi square test was applied to examine the association between dependent and predictor variables like gender and blood donation status.
Ethical consideration
The study was approved by the ethical review committee of Debere Markos University Ethical Review Board. Once the research proposal secured ethical clearance and approval from the university board, the obtained letter from the board was submitted to Addis Ababa city administration health bureau for further review and approval by the regional health bureau ethical committee in line with the their internal procedures. A letter, to go ahead and support the study, was obtained from the city administration health bureau. Verbal consent was obtained from the administration personnel of each health facilities before commencing with the distribution of the self-administered questionnaires to the study participants.
The respondents were briefly informed individually about the study to ensure informed consent was kept. At the same time they were informed that confidentiality will be kept throughout the data collection, the entire study period and beyond. Respondents who were not comfortable to undergo with the questionnaire had given the right to quite the study at any time.
Result
Socio demographic characteristics
A total of 774 individual health care providers were included in this study which resulted with a response rate of 95.8%; of whom 397 (51.3%) being women and the remaining 377 (48.7%) were men. The participants were from both private and government health facilities across the selected sub cities. A mean age of 28.7± 6.5 years were observed in this survey. Majority of respondents who participated in this survey were single 460 (59.4%) of the overall respondents. Orthodox Christianity was the main religion practiced among the respondents which accounted for 511 (66%) followed by Protestant Christianity which constituted 133 (17.2%) of the overall respondents. Majority of the participants 420 (54.3%) had diploma in health and health related fields and the remaining proportion of the respondents had degree. Majority of the respondents had blood type of O+ 150 (42.7%) followed by B+80 (22.8%). Those participants who had for 13 years and above as a health care professionals accounted for 106 (13.7%) (Table 2).
| Characteristics | Frequency (n=774) | Percentage | |
| Gender | Female | 397 | 51.3 |
| Male | 377 | 48.7 | |
| Marital status | Single | 460 | 59.4 |
| Married | 292 | 37.7 | |
| Divorced/Separated | 12 | 1.6 | |
| Widow | 10 | 1.3 | |
| Educational status | Diploma | 420 | 54.3 |
| Degree | 354 | 45.7 | |
| Religion | Orthodox | 511 | 66 |
| Protestant | 133 | 17.2 | |
| Muslim | 87 | 11.2 | |
| Others | 28 | 3.6 | |
| Catholic | 15 | 1.9 | |
| Age group in years | ≤22 | 68 | 8.8 |
| 23-29 | 423 | 54.7 | |
| 30-35 | 185 | 23.9 | |
| ≥36 | 98 | 12.7 | |
| Length of Service as a health care professionalin years | 1-6yrs | 517 | 66.8 |
| 7-12yrs | 151 | 19.5 | |
| ≥13yrs | 106 | 13.7 | |
| Profession | Nurse | 457 | 59 |
| Health Officer | 72 | 9.3 | |
| Lab Tech | 60 | 7.8 | |
| Pharmacy Tech | 58 | 7.5 | |
| Physicians | 41 | 5.3 | |
| Midwife | 39 | 5 | |
| Specialized Nurse | 16 | 2.1 | |
| Health Educator | 11 | 1.4 | |
| Radiology | 11 | 1.4 | |
| Environmental Health | 9 | 1.2 | |
| Department | Inpatient | 243 | 31.4 |
| Outpatient | 237 | 30.6 | |
| Pharmaceutical | 57 | 7.4 | |
| Laboratory | 56 | 7.2 | |
| MCH | 52 | 6.7 | |
| Operation Room (OR) | 38 | 4.9 | |
| Administration | 24 | 3.1 | |
| ART | 22 | 2.8 | |
| Reception/Triage | 20 | 2.6 | |
| EPI | 14 | 1.8 | |
| Radiology | 11 | 1.4 | |
| Blood transfusion services within the facility | No | 549 | 70.9 |
| Yes | 225 | 29.1 | |
| Motivation by someone for blood transfusion | No | 526 | 68 |
| Yes | 248 | 32 | |
| Mass Media exposure towards bloodtransfusion | Yes | 608 | 78.6 |
| No | 166 | 21.4 | |
| HIV tested in the past | Yes | 711 | 91.3 |
| No | 63 | 8.1 | |
| Blood group of respondents | O+ | 150 | 42.7 |
| B+ | 80 | 22.8 | |
| A+ | 62 | 17.7 | |
| AB+ | 36 | 10.3 | |
| O- | 13 | 3.7 | |
| A- | 7 | 2 | |
| B- | 3 | 0.9 |
Table 2: Socio demographic and blood donation related characteristics of health care providers in Addis Ababa Health Facilities, Ethiopia Oct 2014.
Level of KAP towards voluntary blood donation
Knowledge: Knowledge level of individuals was assessed using a number of questions. Among the study participants, 415 (53.6 %) of the respondents did not know how often an individual can donate blood. Twenty eight percent of the respondents did not know their blood group. 354 (46%) of individuals did not know the volume of blood donated at each donation process. Moreover, more than half 417 (53.9 %) of the respondents did not know the duration of a single donation process. Slightly lower than half 346 (44.7%) of the participants were not aware whether hepatitis C virus (HCV) could be potentially transmitted through blood transfusions although 737 (95%) of the respondents are quite aware that HIV could be transmitted through blood transfusion.
The overall level of knowledge was determined by summing up the correct answers of each individual response together. Hence it is found that 72.7% of the respondents have scored more than the 50th percentile of the correct answers in which they are labeled as having adequate knowledge. However, the remaining 27.3% of respondents did not achieve the 50% percentile of the correct answer and hence they are considered as having inadequate knowledge (Table 3).
| Questions | Frequency | Percentage | ||
| (n =774) | ||||
| Knowledge of the common blood groups | Yes | 668 | 86.3 | |
| No | 106 | 13.7 | ||
| Knowledge of your blood group | Yes | 557 | 72.0 | |
| No | 211 | 27.3 | ||
| No Response | 6 | 0.8 | ||
| Blood transfusion can bring infection | Yes | 504 | 65.1 | |
| No | 270 | 34.9 | ||
| Diseases which are transmissible by blood Transfusion |
HIV | Yes | 737 | 95.2 |
| No | 37 | 4.8 | ||
| HCV | Yes | 428 | 55.3 | |
| No | 346 | 44.7 | ||
| Malaria | No | 412 | 53.2 | |
| Yes | 362 | 46.8 | ||
| HBV | Yes | 603 | 77.9 | |
| No | 171 | 22.1 | ||
| Syphilis | Yes | 397 | 51.3 | |
| No | 377 | 48.7 | ||
| Frequency of blood donation in a year | Three monthly | 359 | 46.4 | |
| Six Monthly | 234 | 30.2 | ||
| Do not know | 84 | 10.9 | ||
| Annually | 50 | 6.5 | ||
| Monthly | 34 | 4.4 | ||
| Others | 10 | 1.3 | ||
| Weekly | 3 | 0.4 | ||
| Knowledge of potential blood donors |
Men | Yes | 557 | 72.0 |
| No | 217 | 28.0 | ||
| Women | Yes | 462 | 59.7 | |
| No | 312 | 40.3 | ||
| Healthy | Yes | 488 | 63.0 | |
| No | 286 | 37.0 | ||
| Young<18yrs | No | 705 | 91.1 | |
| Yes | 69 | 8.9 | ||
| Old>60yrs | No | 757 | 97.8 | |
| Yes | 17 | 2.2 | ||
| Vulnerable group | No | 689 | 89.0 | |
| Yes | 85 | 11.0 | ||
| Diseased | No | 749 | 96.8 | |
| Yes | 25 | 3.2 | ||
| Knowledge regarding who should not donate | Men | No | 741 | 95.7 |
| Yes | 33 | 4.3 | ||
| Women | No | 733 | 94.7 | |
| Yes | 41 | 5.3 | ||
| Healthy | No | 732 | 94.6 | |
| Yes | 42 | 5.4 | ||
| Young<18yrs | Yes | 421 | 54.4 | |
| No | 353 | 45.6 | ||
| Old>60yrs | Yes | 420 | 54.3 | |
| No | 354 | 45.7 | ||
| Vulnerable group | No | 604 | 78.0 | |
| Yes | 170 | 22.0 | ||
| Diseased | Yes | 516 | 66.7 | |
| No | 258 | 33.3 | ||
| Cultural Belief | No | 741 | 95.7 | |
| Yes | 33 | 4.3 | ||
| Religious Belief | No | 735 | 95.0 | |
| Yes | 39 | 5.0 | ||
| Volume of blood collected during each donation | <500mls | 420 | 54.3 | |
| 500-1000mls | 263 | 34.0 | ||
| Don’t know | 91 | 11.7 | ||
| Duration of a donation process | 20-60 minutes | 357 | 46.1 | |
| <20 minutes | 218 | 28.2 | ||
| Do not know | 199 | 25.7 |
Table 3: Level of knowledge toward blood donation among health care workers in Addis Ababa health facilities Ethiopia, October 2014.
Attitude: among the overall respondents 715 (92.3 %) of respondents of the survey said blood donation is good, whereas 14 (1.8%) thinks bad. Similarly 590 (76.2%) of individuals responded as voluntary blood donation is the best source of blood. Majority 488 (63%) of respondents think that relatives of patient should be asked for blood donation. The overall attitude of individuals towards voluntary blood donation was assessed by summing up the correct answers of individual questions. In this study it was observed that 633 (81.7%) of respondents have a positive attitude towards blood donation. The remaining segment being unfavorable attitude towards VBD (Table 4).
| Questions | Frequency | Percent | |
| What do you think about Blood donation? | Good | 715 | 92.38 |
| Neutral | 45 | 5.81 | |
| Bad | 14 | 1.81 | |
| What do you think is the best source of blood? | Voluntary donor | 590 | 76.23 |
| Replacement donor | 105 | 13.57 | |
| Self-donor | 46 | 5.94 | |
| Do not know | 29 | 3.75 | |
| Remunerated donor | 4 | 0.52 | |
| Can something harmful happen to a blood donor? | Yes | 257 | 33.20 |
| NO | 517 | 66.80 | |
| What can happen to a blood donor during or after donation? |
Temporary Weakness | 656 | 84.75 |
| Contract Infection | 91 | 11.76 | |
| Fall Sick | 27 | 3.49 | |
| Should patient relatives be asked to donate? | Yes | 488 | 63.05 |
| No | 244 | 31.52 | |
| Do not Know | 42 | 5.43 |
Table 4: Level of attitude towards blood donation among health care workers in Addis Ababa health facilities, Ethiopia, October 2014.
Practice: As far as blood donation practice of respondents is concerned, 252 (32.6%) has ever donated blood at least once in their life time and the remaining 522 (67.4%) never exercised any blood donation practice so far. Moreover, only 121 (15.6%) of the respondents reported to have had blood donated based on voluntarism; whereas about 120 (47.6) of the donors went to donate for their relatives or friends who needed blood. Remuneration donors accounted for 1 (0.39%) of the blood donors. 20 (7.93%) of the overall donors are regular blood donors. However, the proportion of regular blood donors among the study participants was only 2.6%.
More than two thirds 536 (69.2%) of the participants were willing to donate blood in the future if they are called upon or reminded to do so and 198 (25.6%) of the respondents would not like to give blood in future. The remaining 40 (5.17%) of the respondents were not sure if they could donate blood in future. As noted from Table 5, the main reasons for not donating blood by the non-donors were; not approach/ asked to donate, need to donate in future for relatives or friends and fear of knowing my status with proportion of 40.9%, 17.8% and 9.9% respectively. 4.9% of the non-donors pointed out that the reason for not donating blood was because there is no remuneration.
| Questions | Answers | Frequency(n=774) | Percent |
| Have you ever donated blood inyour life | Yes | 252 | 32.56 |
| No | 522 | 67.44 | |
| How often do you donate | <1 time a year 1–3 times a year >3 times a year |
192 | 24.81 |
| 40 | 5.17 | ||
| 20 | 2.58 | ||
| Why did you donate | Voluntary | 121 | 15.63 |
| To know my screening status | 10 | 1.29 | |
| Remuneration | 1 | 0.13 | |
| A friend or relative needed blood | 120 | 15.50 | |
| Will you donate if called upon or reminded to do so |
Yes | 536 | 69.25 |
| No | 198 | 25.58 | |
| Do not know | 40 | 5.17 | |
| Reasons for Non donation by non- donors (n=522) |
Religion forbids it | 31 | 5.94 |
| No remuneration | 26 | 4.98 | |
| Need to donate for friends or | 93 | 17.82 | |
| relatives in future | |||
| Fear of knowing my status | 52 | 9.96 | |
| Unfit to donate | 46 | 8.81 | |
| Not approached to donate | 213 | 40.80 | |
| Fear of needles | 27 | 5.17 | |
| Donated blood may be sold | 16 | 3.07 | |
| No response | 18 | 3.45 |
Table 5: Level of blood donation practice among health care workers in Addis Ababa health facilities, Ethiopia, October 2014.
Factors associated with knowledge towards blood donation
Bivariate and multivariate analysis was computed to determine factors that were associated with level of knowledge of the health care providers. As can be seen in Table 3, nine variables showed significant association with knowledge level of blood donation at a 5% level of significant fulfilling the minimum requirement of 0.2 level of significance for further analysis. However; the remaining three variables such as department of respondents, previous HIV test status and profession did not show any significance association at 0.2 level of significance, hence those variables were excluded from further analysis. Those predictor variables that fulfilled the minimum requirements were entered to the multivariate analysis and further analysed.
Therefore, it was noted that having 13 years (and above) experience as a health care professional is likely to acquire 13.5 times more knowledge than 1-6years experience (AOR=13.57, 95%CI: 4.89, 37.68). In addition to this, those individuals who have been working between 7 and 12 years are likely to have about 2 times more knowledge than 1-6 years of experience (AOR=1.81, 95% CI: 1.17, 2.79). Similarly availability of blood transfusion services within the facility is likely to increase the knowledge level of BD by 2.9 times as compared to those who did not have (AOR=2.89, 95%CI: 1.90, 4.41).
Respondents who have been exposed to mass media about Voluntary blood donation were found to be statically significant predictors of levels of knowledge at (AOR=1.91, 95%CI: 1.29, 2.82). Hence those group of individuals who had previous mass media exposure about blood donation were likely to have about two times more knowledge than non-exposed groups (Tables 6 and 7).
| Knowledge level | 95% Confidence | |||||
| Interval | ||||||
| Variable | Inadequate | Adequate | Odds Ratio (Crude) |
Lower | Upper | |
| Gender | Female | 117 | 280 | 1 | - | - |
| Male | 93 | 284 | 1.276 | 0.928 | 1.754 | |
| Marital status | Divorced/Separated | 2 | 10 | 1 | - | - |
| Married | 66 | 226 | 2.143 | 0.281 | 16.369 | |
| Single | 139 | 321 | 1.468 | 0.369 | 5.833 | |
| Widow | 3 | 7 | 0.99 | 0.252 | 3.883 | |
| Educational status | Degree | 80 | 274 | 1 | ||
| Diploma | 130 | 290 | 0.651 | 0.471 | 0.9 | |
| Age group | 23-29 | 25 | 43 | 1 | ||
| 30-35 | 135 | 288 | 1.24 | 0.727 | 2.115 | |
| ≥36 | 44 | 141 | 1.863 | 1.025 | 3.388 | |
| ≤22 | 6 | 92 | 8.915 | 3.407 | 23.324 | |
| Religion | Catholic | 8 | 7 | 1 | ||
| Muslim | 24 | 63 | 3 | 0.981 | 9.176 | |
| Orthodox | 131 | 380 | 3.315 | 1.179 | 9.32 | |
| Protestant | 37 | 96 | 2.965 | 1.004 | 8.758 | |
| Others | 10 | 18 | 2.057 | 0.575 | 7.364 | |
| Service year as a health careprofessional | 1-6yrs | 172 | 345 | 1 | - | - |
| 7-12yrs | 34 | 117 | 1.716 | 1.123 | 2.62 | |
| ≥13yrs | 4 | 102 | 12.713 | 4.604 | 35.102 | |
| Profession | Environmental | 5 | 4 | 1 | - | - |
| Health | - | - | - | - | - | |
| Health Educator | 1 | 10 | 12.5 | 1.089 | 143.432 | |
| Health Officer | 22 | 50 | 2.841 | 0.696 | 11.603 | |
| Lab Technician | 18 | 42 | 2.917 | 0.701 | 12.139 | |
| Physicians | 5 | 36 | 9 | 1.793 | 45.187 | |
| Midwife | 12 | 27 | 2.812 | 0.64 | 12.358 | |
| Nurse | 123 | 334 | 3.394 | 0.897 | 12.846 | |
| Pharmacy Tech | 17 | 41 | 3.015 | 0.721 | 12.613 | |
| Radiology | 3 | 8 | 3.333 | 0.515 | 21.584 | |
| Specialized Nurse | 4 | 12 | 3.75 | 0.662 | 21.252 | |
| Department | Administration | 5 | 19 | 1 | ||
| ART | 4 | 18 | 1.267 | 0.309 | 5.201 | |
| EPI | 3 | 11 | 1.5 | 0.341 | 6.607 | |
| Inpatient | 71 | 172 | 1.222 | 0.24 | 6.233 | |
| Laboratory | 18 | 38 | 0.808 | 0.283 | 2.306 | |
| MCH | 15 | 37 | 0.704 | 0.221 | 2.238 | |
| OR | 7 | 31 | 0.822 | 0.254 | 2.667 | |
| Outpatient | 64 | 173 | 1.476 | 0.401 | 5.431 | |
| pharmaceutical | 16 | 41 | 0.901 | 0.315 | 2.58 | |
| Radiology | 2 | 9 | 0.854 | 0.266 | 2.74 | |
| Reception/Triage | 5 | 15 | 1.5 | 0.239 | 9.41 | |
| Motivation by colleagues to donateblood | No | 158 | 368 | 1 | - | - |
| Yes | 52 | 196 | 1.618 | 1.131 | 2.315 | |
| Mass Media exposure towards bloodtransfusion | No | 59 | 107 | 1 | - | - |
| Yes | 151 | 457 | 0.599 | 0.415 | 0.865 | |
| Tested for HIV | No | 19 | 26 | 1 | ||
| Yes | 191 | 538 | 0.784 | 0.45 | 1.367 | |
| Blood transfusion services within thefacility | No | 176 | 373 | 1 | - | - |
| Yes | 34 | 191 | 2.651 | 1.765 | 3.98 | |
Table 6: Results of bivariate analyses of predictor variables towards knowledge level among health care providers in Addis Ababa health facilities, Ethiopia, Oct 2014.
| Knowledge level | 95% CI | |||||
| Explanatory variables | Inadequate | Adequate | Odds Ratio(Adjusted) | Lower | Upper | |
| Service year as a health careprofessional | 1-6yrs | 172 | 345 | 1 | ||
| 7-12yrs | 34 | 117 | 1.81 | 1.173 | 2.794 | |
| ≥13yrs | 4 | 102 | 13.573 | 4.889 | 37.686 | |
| Availability of Blood transfusionservices in the facility | No | 176 | 373 | 1 | ||
| Yes | 34 | 191 | 2.896 | 1.904 | 4.405 | |
| Mass Media exposure towards bloodtransfusion | No | 59 | 107 | 1 | - | - |
| Yes | 151 | 457 | 1.908 | 1.289 | 2.824 | |
Table 7: Factors associated with knowledge level of health care workers towards voluntary blood donation in Addis Ababa health facilities, Ethiopia, October 2014.
Factors associated attitude towards voluntary blood donation
Five of the twelve variables did not show a significance association with the outcome variables at 5% level of significance. Results of separately regressed variables indicated that ,Marital status, Profession, Motivation by colleagues/someone for blood transfusion, Mass Media exposure towards blood transfusion and HIV test status of respondents were not significant at 0.2 level of significance as a result of this they were excluded from further analysis. Nevertheless the remaining seven variables were found to be significant at 0.2 level of significance and hence a collective further analysis was required using multivariate analysis to control the possible confounders among the predictors. But at this stage it is only two variables, gender and age group remained to be significantly and independently associated with the level of attitude (Tables 8 and 9).
| Predictor variables | Attitude | OR (crude) |
95% C.I. | |||
| Unfavorable | Favorable | Lower | Upper | |||
| Gender | Female | 99 | 298 | 1 | ||
| Male | 43 | 334 | 2.614 | 1.764 | 3.875 | |
| Marital status | Divorced/Separated | 2 | 10 | 1 | - | - |
| Married | 52 | 240 | 0.556 | 0.043 | 7.214 | |
| Single | 87 | 373 | 0.513 | 0.064 | 4.136 | |
| Widow | 1 | 9 | 0.49 | 0.061 | 3.921 | |
| 53 | 301 | - | - | - | ||
| Educational status | Degree | - | - | 1 | - | - |
| Diploma | 89 | 331 | 1.539 | 1.056 | 2.243 | |
| Age Group | ≤22 | 19 | 49 | 1 | ||
| 23-29 | 90 | 333 | 1.455 | 0.816 | 2.596 | |
| 30-35 | 24 | 161 | 2.731 | 1.375 | 5.426 | |
| ≥36 | 9 | 89 | 3.834 | 1.612 | 9.119 | |
| Service year as a health care professional |
1-6 Years | 109 | 408 | 1 | ||
| 7-12 years | 23 | 128 | 1.654 | 0.996 | 2.746 | |
| ≥13 years | 10 | 96 | 2.565 | 1.293 | 5.086 | |
| Profession | Environmental Health | 2 | 7 | 1 | - | - |
| Health Educator | 2 | 9 | 0.5 | 0.058 | 4.335 | |
| Health Officer | 15 | 57 | 0.643 | 0.076 | 5.417 | |
| Lab Tech | 8 | 52 | 0.543 | 0.111 | 2.654 | |
| Physicians | 4 | 37 | 0.929 | 0.177 | 4.874 | |
| Midwife | 6 | 33 | 1.321 | 0.217 | 8.037 | |
| Nurse | 87 | 370 | 0.786 | 0.141 | 4.379 | |
| Pharmacy Tech | 12 | 46 | 0.608 | 0.136 | 2.723 | |
| Radiology | 2 | 9 | 0.548 | 0.109 | 2.745 | |
| Specialized Nurse | 2 | 14 | 0.643 | 0.076 | 5.417 | |
| Department | Administration | 5 | 19 | 1 | - | - |
| ART | 1 | 21 | 0.95 | 0.218 | 4.146 | |
| EPI | 7 | 7 | 5.25 | 0.534 | 51.626 | |
| Inpatient | 43 | 200 | 0.25 | 0.055 | 1.138 | |
| Laboratory | 8 | 48 | 1.163 | 0.37 | 3.651 | |
| MCH | 10 | 42 | 1.5 | 0.398 | 5.654 | |
| OR | 3 | 35 | 1.05 | 0.288 | 3.832 | |
| Outpatient | 44 | 193 | 2.917 | 0.583 | 14.585 | |
| pharmaceutical | 13 | 44 | 1.097 | 0.349 | 3.441 | |
| Radiology | 2 | 9 | 0.846 | 0.24 | 2.978 | |
| Reception/Triage | 4 | 16 | 1.125 | 0.171 | 7.399 | |
| Religion | Catholic | 8 | 7 | 1 | - | - |
| Muslim | 17 | 70 | 3.883 | 1.229 | 12.266 | |
| Orthodox | 86 | 425 | 4.324 | 1.528 | 12.24 | |
| Others | 5 | 23 | 4.025 | 0.991 | 16.347 | |
| Protestant | 26 | 107 | 3.601 | 1.197 | 10.831 | |
| Blood transfusion services within the facility |
No | 108 | 441 | 1 | - | - |
| Yes | 34 | 191 | 1.344 | 0.882 | 2.05 | |
| Motivation by colleagues to donate blood |
No | 100 | 426 | 1 | ||
| Yes | 42 | 206 | 1.123 | 0.754 | 1.672 | |
| Mass Media exposure towards blood transfusion |
No | 33 | 133 | 1 | - | - |
| Yes | 109 | 499 | 1.162 | 0.752 | 1.794 | |
| Tested for HIV | No | 10 | 35 | 1 | - | - |
| Yes | 132 | 597 | 1.048 | 0.532 | 2.064 |
Table 8: Results of bivariate analyses of predictor variables towards attitude of VBD among health care providers in Addis Ababa health facilities, Ethiopia, Oct 2014
| Attitude | 95%C.I. | |||||
| Variables | Unfavorable | Favorable | OR (Adjusted) | Lower | Upper | |
| Gender | Female | 99 | 298 | 1 | ||
| Male | 43 | 334 | 2.348 | 1.572 | 3.509 | |
| Age Group | ≤22 | 19 | 49 | 1 | - | - |
| 23-29 | 90 | 333 | 1.234 | 0.685 | 2.225 | |
| 30-35 | 24 | 161 | 2.105 | 1.044 | 4.245 | |
| ≥36 | 9 | 89 | 2.872 | 1.189 | 6.936 | |
Table 9: Factors associated with attitude of health care workers towards voluntary blood donation in Addis Ababa health facilities, Ethiopia, October 2014.
Multivariate analysis indicated that being male is significantly associated and increased odd of favorable attitude (AOR=2.35, 95%CI: 1.57, 3.51). Hence men were more likely to have 2.4 times favorable attitude towards voluntary blood donation than females. On the other hand older age groups of the participants are significantly associated with positive attitudes towards voluntary blood donation. Having age ≥36 years was likely to have 2.9 times favorable attitude compared to the age group ≤22 years (AOR=2.9, 95%CI: 1.19, 6.94). Similarly those groups of individuals with age range between 30 and 35 (inclusive) were more likely to have 2.1 times favorable attitude than ≤22 years of age (AOR=2.12, 95% CI: 1.04, 4.25). However the age group between 23 and 29 did not show any difference compared with ≤22 years in terms of attitude status.
Factors associated with practice of blood donation
As can be noted from the bivariate and multivariate analysis as shown below in Tables 7 and 8, four of the thirteen predictor variables did not show significance to the outcome variable at 5% level of significance. Department, religion, Mass Media exposure towards blood donation and previous HIV test status were excluded from analysis since they did not show any significance at 0.2 level of significance when regressed separately. Among the variables which were analyzed using multivariate logistic regression, age group and education status have been removed since they did not have association with the outcome variable at 5% level of significance.
A multivariate analysis (Table 10) on blood donation practice revealed a statistical significant association with gender. Males were 2.2 times more likely to practice blood donation than females (AOR=2.25, 95% CI: 1.52, 3.26). Knowledge over VBD was found to have had a significant association with Blood donation practice. Respondents with adequate knowledge over voluntary blood donation were found to be four times more likely to practice blood donation than those individuals with inadequate knowledge (AOR=4.38, 95%CI: 2.54, 7.56). Likewise those group of individuals who have been working more than 13 years are 4.6 times more likely to exercise blood donation practice than those individual who have been working between 1 and 6 years (AOR=4.61, 95% CI:1.71, 12.38)
| Characteristics | BD Practice | 95% C.I. | ||||
| No | Yes | OR(Crude) | Lower | Upper | ||
| Gender | Female | 306 | 91 | 1 | - | - |
| Male | 216 | 161 | 2.506 | 1.837 | 3.419 | |
| Marital status | Divorced/Separated | 6 | 6 | 1 | - | - |
| Married | 172 | 120 | 0.698 | 0.22 | 2.215 | |
| Single | 338 | 122 | 0.361 | 0.114 | 1.14 | |
| Widow | 6 | 4 | 0.667 | 0.122 | 3.64 | |
| Educational status | Degree | 207 | 147 | 1 | - | - |
| Diploma | 315 | 105 | 0.469 | 0.346 | 0.637 | |
| Age Group in years | ≤22 | 55 | 13 | 1 | - | - |
| 23-29 | 332 | 91 | 1.16 | 0.607 | 2.216 | |
| 30-35 | 106 | 79 | 3.153 | 1.612 | 6.168 | |
| ≥36 | 29 | 69 | 10.066 | 4.784 | 21.182 | |
| Service year as a health care professional | 1-6 years | 401 | 116 | 1 | - | - |
| 7-12 years | 93 | 58 | 2.156 | 1.463 | 3.177 | |
| ≥13 years | 28 | 78 | 9.63 | 5.967 | 15.542 | |
| Profession | Environmental Health | 6 | 3 | 1 | - | - |
| Health Educator | 7 | 4 | 1.143 | 0.179 | 7.283 | |
| Health Officer | 44 | 28 | 1.273 | 0.294 | 5.506 | |
| Lab Tech | 33 | 27 | 1.636 | 0.374 | 7.162 | |
| Physicians | 17 | 24 | 2.824 | 0.618 | 12.894 | |
| Midwife | 25 | 14 | 1.12 | 0.242 | 5.186 | |
| Nurse | 328 | 129 | 0.787 | 0.194 | 3.192 | |
| Pharmacy Tech | 43 | 15 | 0.698 | 0.155 | 3.144 | |
| Radiology | 10 | 1 | 0.2 | 0.017 | 2.386 | |
| Specialized Nurse | 9 | 7 | 1.556 | 0.284 | 8.531 | |
| Department | Administration | 13 | 11 | 1 | - | - |
| ART | 14 | 8 | 0.675 | 0.207 | 2.204 | |
| EPI | 8 | 6 | 0.886 | 0.235 | 3.347 | |
| Inpatient | 176 | 67 | 0.45 | 0.192 | 1.053 | |
| Laboratory | 30 | 26 | 1.024 | 0.392 | 2.674 | |
| MCH | 35 | 17 | 0.574 | 0.213 | 1.545 | |
| OR | 23 | 15 | 0.771 | 0.274 | 2.166 | |
| Outpatient | 158 | 79 | 0.591 | 0.253 | 1.379 | |
| Pharmaceutical | 42 | 15 | 0.422 | 0.156 | 1.143 | |
| Radiology | 9 | 2 | 0.263 | 0.047 | 1.481 | |
| Reception/Triage | 14 | 6 | 0.506 | 0.145 | 1.766 | |
| Religion | Catholic | 13 | 2 | 1 | - | - |
| Muslim | 59 | 28 | 3.085 | 0.651 | 14.609 | |
| Orthodox | 338 | 173 | 3.327 | 0.742 | 14.909 | |
| Others | 21 | 7 | 2.167 | 0.389 | 12.063 | |
| Protestant | 91 | 42 | 3 | 0.648 | 13.895 | |
| Motivation by someone to donate blood | No | 385 | 141 | 1 | - | - |
| Yes | 137 | 111 | 2.212 | 1.613 | 3.035 | |
| Mass media exposure radio TV about blood donation | No | 112 | 54 | 1 | - | - |
| Yes | 410 | 198 | 1.002 | 0.694 | 1.445 | |
| Tested for HIV | No | 45 | 18 | |||
| Yes | 477 | 234 | 1.226 | 0.695 | 2.165 | |
| Blood transfusion service within the facility | No | 422 | 127 | 1 | - | - |
| Yes | 100 | 125 | 4.154 | 2.988 | 5.774 | |
| Knowledge | Adequate | 191 | 19 | - | - | - |
| Inadequate | 331 | 233 | 7.076 | 4.29 | 11.671 | |
Table 10: Results of bivariate analyses of predictor variables towards voluntary blood donation practice among health care providers in Addis Ababa health facilities, Ethiopia, Oct 2014.
On the other hand, those groups of individuals who have been working between 7 and 12 years did not have a significance difference with individuals worked between one and six years. Moreover, availability of blood transfusion service within the facility raised the odds of blood donation practices by about 4 times compared to the ones which did not have (OR=4.09, 95% CI: 2.71, 6.16).
Similarly motivation/encouraging by someone like colleagues for blood donation activities showed a significant statistical association with practice of blood donation. Hence those group of individuals who had been motivated by friends or colleagues for blood donation activities raised the odds of donation by about 2 times compared with those group who had not been motivated by colleagues (OR=1.69, 95% CI:1.13, 2.54) (Table 11).
| Variables | Blood Donation Practice |
95% C.I. | ||||
| No | Yes | OR(Adjusted) | Lower | Upper | ||
| Gender | Female | 306 | 91 | 1 | - | - |
| Male | 216 | 161 | 2.246 | 1.549 | 3.257 | |
| Service year as a health careprofessional | 1-6 years | 401 | 116 | 1 | - | - |
| 7-12 years | 93 | 58 | 1.184 | 0.662 | 2.12 | |
| ≥13 years | 28 | 78 | 4.613 | 1.719 | 12.38 | |
| Motivation by someone to donate blood | No | 385 | 141 | 1 | - | - |
| Yes | 137 | 111 | 1.692 | 1.129 | 2.535 | |
| Blood transfusion service within thefacility | No | 422 | 127 | 1 | - | - |
| Yes | 100 | 125 | 4.086 | 2.712 | 6.156 | |
| Knowledge | Inadequate | 191 | 19 | 1 | - | - |
| Adequate | 331 | 233 | 4.389 | 2.549 | 7.556 | |
Table 11: Factors associated with voluntary blood donation practice among health care workers in Addis Ababa health facilities, Ethiopia, October 2014.
Discussion
In line with the objective of the study, an effort was made to find out the level of Knowledge, attitude and practice (KAP) and their respective associated factors towards voluntary blood donation of health care workers in Addis Ababa health facilities.
There are quite a number of studies on KAP towards blood donation that have been published and available online but unfortunately published studies particularly on health care providers are rarely available. It was found that the proportion of males (64%) who have donated blood in this study is significantly higher than females (36%). This finding is supported by studies conducted in the developing world where they found out a greater proportion of males were involved in blood donation than females [22,24].
The present study revealed a significant proportion of health care providers having a good knowledge on blood donation. The cumulative knowledge was about 73% which is less than the results of a previous similar study conducted among Nigerian physicians in Benin City tertiary hospital (93.9%). This is probably because of the difference of the study participants where all respondents in the Nigerian study were physicians, while the present study considers all range of health professionals from the lowest to highest level of education [10].
The level of knowledge on the present study is significantly higher than the findings of the study by Mullah assessing the knowledge and perception of healthcare support staffs of a tertiary healthcare facility in Gujarat where the overall acceptable knowledge level turned out to be 51.6%. This is perhaps because of the respondents were a health care support staff members in which they are likely to be informed lesser compared to be the health care professionals [19].
Similarly the finding of the current study has got significantly higher knowledge level than a study conducted in Thailand where only 42.7% the overall respondents acquired good knowledge [20].
The overall knowledge of respondents in the present study is significantly greater than when it is compared to a study conducted in India where the cumulative knowledge was observed to be about 43%. Again a Similar study on medical and paramedical staff in tertiary institution in Nigeria revealed that a relatively lesser proportion (64.8%) of the respondents had good knowledge about blood donation. This is perhaps mainly due to the para medics are included in the study subjects where the awareness of VBD level is expected to be lesser compared to the present study in which the study subjects have exclusively medical backgrounds [10]. In the present study it was observed that existence of blood transfusion services within the facility, having longer years of service as a health care professional, being exposed to mass media about blood donation and those individuals who have been tested for HIV in the past increased the odds of having adequate knowledge. Availability of blood transfusion service in an institution increases the day to day exposure of individuals with the routine activities dealt with blood transfusions procedures which in turn lead to acquire a better knowledge of the blood transfusion process. Since Mass media exposure regarding BD creates more awareness to individuals, it is logical to observe blood donation campaigns and sensitization through different Medias are directly proportional with the level of the overall knowledge of individuals. In the same way, working for longer period of years as health care professional would give a higher chance of gaining knowledge through experience from the day today activities. This is in agreement with a study carried out in India [22].
In the present study department and profession of respondents did not show statistical significance with level of knowledge although a study among medical students in AAU revealed statistically significant association between department and level of knowledge [24]. The reason that this study did not show statistical association between departments and knowledge level could be the HCWs have a tendency to get exposed with blood transfusion activities regardless of the department in which they are working for. However, knowledge of medical students is often dependent on when they are exposed to the course related to blood transfusion which is not the case for all departments.
In this survey 81.7% of respondents have a positive attitude towards blood donation which is almost equivalent to a study performed in south India where 87.3% of respondents turned out to have a positive attitude towards blood donation but more than what was reported among AAU Medical students with a study conducted in which only about 68% of the respondents had favorable attitude towards blood donation [30].
A statistical significant association is observed between gender and attitude where being male increased the odds of having a positive attitude towards blood donation. This is also supported by a study conducted in Ethiopian Medical School students at Addis Ababa University [24]. This is probably because men are perceived to be the ones that should donate blood since women might have chances of being ineligible because of conditions like breast feeding and pregnancy. In addition to this, older age groups are statistically associated with favorable attitude of respondents. Nevertheless, in contrast to the present study gender did not show any statistical significance with attitude in previous study done in India [30].
In this study it was found out that 32.6% of individuals have ever donated blood at least once in their life time. Whereas a study on health care workers (medic and para medic) in Nigeria shows a blood donation practice of only 22.1% which is lower than the current findings. This could be because the respondents in the Nigerian study were a combination of medics and para medics. It was also reported that about 14% of among Indian and 11% Thai students were ever participated in blood donation activities at least once in their life time which is significantly lower than the current findings. 23.4% of the Ethiopian Medical students in AAU ever participated in blood donation activity. In general lower proportion of blood donation practices among students than HCWs was noted [5,10,20,24].
It was also observed that the proportion of family/relative replacement blood donors accounted for about 50% of the overall donors which is in agreement with a study conducted among Nigerian health care workers where 52.8% of the donors were noted as family replacement and a bit higher compared to a study in India where the proportion of voluntary donation was 44% [10,16].
On the same hand, in agreement with the present study, a relatively equivalent proportion of blood donation practice (48%) were observed in a similar study conducted in south India in contrary to a KAP survey done in KPU college where a blood donation practice found to be 24 % [24,31].
It was observed that the proportion of voluntary blood donation among KPU medical students in India were 13.3% which is in agreement with the present study (15.6%) but higher than the ones in the Nigerian health care workers where VBD rate was fond out to be 9.2%. However, it is less than when it is compare with national average reported in 2010 (23.5%) [10,24].
In the present study regular voluntary blood donors’ accounted for 7.9% of the overall donors which shows a bigger disparity compared with what was reported in India where 3.3% of Indian medical students were participated in voluntary blood donation activities. 39.6% of Nigerian health care workers were also reported to have participated in voluntary blood a donation activity which is significantly higher than the current finding. An encouraging figure (42.2%) of voluntary blood donation practice were reported among Ethiopian Medical students were in the [10,24].
In the present study, the main reason for not donating blood by non-donors was reported to be because of no one has asked the respondents to donate blood which is in agreement with other findings in Nigerian studies. Respondents would go for VB donation if they were approached by someone to donate blood. This is also supported by a number of studies in the developing world [10,16,31].
In the present study it was found out that predominantly males were the major sources of blood donation more than females which is supported by a number of many other studies in Sub Saharan Africa and India [10,27,32-34].
However, in contrary to this, a study conducted in south-western Spain, revealed that 52.3% of donors were women compared to 47.7% of men. Other studies in developed world documented similar findings [33,34].
The current study also revealed a significant association between blood donation and gender. Although women are potential blood donors, there are a number of circumstances where they could not be as eligible as men like lactations and pregnancy may matter.
Gender, Service year as a health care professional, availability of blood transfusion services within the facility and Knowledge level of the respondents were found to be the most independently determinant factors of voluntary blood donation practice.
Individuals with longer years of service as a health care professionals is likely to come across with occasions where there is a need to donate blood than those individuals working just for few years. Similarly, individuals working in a facility where blood transfusion services are available are likely to be aware more about the importance of blood donation and subsequently they are likely to donate blood. Finally, as someone would anticipate, having adequate knowledge on voluntary blood donation leads the individuals to practice voluntary blood donation than individuals who have not had adequate knowledge.
Limitation
This study was able to illustrate the most determinant factors of KAP towards voluntary blood donation among a range of health care providers despite the fact that it was accompanied by a a certain short comings.
The study was cross-sectional and hence a temporal relationship between predictors and outcome variables cannot be established. It was also not possible to verify fully whether the respondents completed the questionnaire without assistance from colleagues. This is because some of the respondents were too busy to complete the questionnaires at the spot and needed to wait till they have time to do it.
Although there are a number of published literatures across Asian continent and the developing world on KAP of voluntary blood donation, it is barley available on a study conducted on health care providers. Moreover local published literatures regarding the knowledge, attitude and practice of blood donations are hardly available regardless of which study subjects they are dealing with.
Conclusion
The level of knowledge towards blood donation is not as high as someone would anticipant considering the fact that the study participants are health care professional in which they are expected to be more informed than anyone else. There was a good level of favorable attitude observed among the respondents. Blood donation practice is low compared to WHO standards; particularly the level of voluntary blood donation and regular donation is very low. Gender, availability of blood transfusion services and greater service years are associated with blood donation excise of respondents.
Acknowledgements
I would like to express my deepest gratitude for my advisor, Mr.Muluken Dessalegn, who has been helping me and giving directions during the entire period of this proposal development and report preparation. Without his constant advice, this study would not have been materialized.
Last but not least, I am very much grateful to the study participants for being willing to participate and consumed a non-negligible amount of their time to fill up and complete all the questions in the questionnaires.
Assurance of Principal Investigator and Mentor
I the undersigned agree to accept all responsibilities for the scientific and ethical conduct of the research project and for the provision of required progress reports as per terms and conditions of the research publications office in effect at the time of grant is forwarded as the result of this application
Recommendation
Following the findings of the study, the following recommendations were made;
• Create more awareness and sensitization of the health care workers to wards blood donation-makes more sense if it is organized on regular bases.
• Encourage, recruit and motivate potential donors including health care workers in order to have a pool of eligible donors
• Organize social events ones in a year that could approach health care providers and initiate blood donations
• More and more studies need to be conducted on this matter to identify more gaps and perhaps possible interventions accordingly.
References
- The American Red Cross, History of blood transfusion 2013
- Blood safety and availability WHO Fact sheet, Fact sheet N°279, 2014
- Tobler LH, Busch MP (1997) History of post transfusion hepatitis. Clinical Chemistry43: 1487-1493
- Voluntary blood donation towards safe and healthy living (2014). The International Federation of Red Cross and Red Crescent Societies (IFRC)
- Pravin NY, Keerti SJ (2013) A cross-sectional study on knowledge, attitude and practice on blood donation among medical students of South India. International journal of medical and health sciences 2: 2277-2281.
- WHO global data base. Blood safety (2012)
- The Ethiopian Red Cross society national blood bank. Health care blood bank 2012
- World Health Organization (WHO) Report Cooperation Strategy 2012-2015 Ethiopia - data reported by WHO (2013).
- Federal Ministry of Health, Infection Prevention guidelines (2004), blood bank and transfusion services.
- Benedict N, Usimenahon A, Alexander N (2013) Knowledge, Attitude, and Practice of Voluntary Blood Donation among Healthcare Workers at the University of Benin Teaching Hospital, Benin City, Nigeria. Journal of Blood Transfusion 10: 115-120
- Ministry of Health, Health Sector Development Program of Ethiopia (HSDP) IV 2010/11-2014/15
- Centers for disease control and prevention (CDC) report (2011) Progress towards Strengthening National Blood Transfusion Services - 14 Countries report, 2008-2010. 60: 1578-1582
- Federal democratic republic of Ethiopia, ministry of health. National blood transfusion Services strategy (2005) .
- Central Statistical Agency report, Ethiopia demographic and health survey (2011).
- The Melbourne declaration on 100% voluntary non-remunerated donation of blood and blood components,” Composed at World Blood Donor Day. Melbourne, Australia (2009).
- Amit A, Amit G, Gauravi D, Kakadia M (2014) Knowledge, attitude, and practice of voluntary blood donation among medical students of PDU medical college India Rajkot. International Journal of Current Research 6: 6839-6841.
- Javadzadeh SH, Yavari MT, Attar M, Ahmadiyeh MH (2004) Knowledge, attitude and practice study about donation in the urban population of Yazd, Iran. Transfus Med 1: 403-405
- Mullah F, Kumar D, Antani D, Gupta M (2013 ) Study of knowledge, perceptions and practices related to blood donation among the healthcare support staff of a tertiary care hospital in Gujarat, India .The Online Journal of Health and Allied Sciences 12: 618-630.
- Wiwanitkit V (2002) Knowledge about blood donation among a sample of Thai university students. Vox Sang 83: 97-99
- Shenga N, Pal R, Sengupta S (2008) Behavior disparities towards blood donation in Sikkim, India. Asian J Transfus Sci 2: 56-60
- Amit A, Aseem KT, Alok A, Rakesh K (2013) Knowledge, attitude and practices of people towards voluntary blood donation in Uttarakhand. Asian Journal of transfusion science 7: 59-62
- Salaudeen AG, Odeh E (2011) Knowledge and behavior towards voluntary blood donation among students of a tertiary institution in Nigeria. Nigerian Journal of clinical practice 14: 303-307
- Misganaw C, Tenkir M, Deresea A, Tesfaye M, Hawult T (2014)The level and associated factors of knowledge, attitude and practice of blood donation among health science students of Addis Ababa University. International Journal of Medical and Health Sciences Research 1: 105-118.
- Manikandan S, Srikumar R, Ruvanthika PN (2013) A Study on Knowledge, Attitude and Practice on Blood Donation among Health Professional Students in Chennai, Tamil Nadu, South India. International Journal of Scientific and Research Publications 3: 2250-2253
- Purushottam AG, Deepak BP (2012) Knowledge and Attitude about Blood Donation Amongst Undergraduate Students of Pravara Institute of Medical Sciences Deemed University of Central India. Annals of Tropical Medicine and Public Health 5: 569-573.
- Vasquez M, Ibarra P, Maldonado M (2007) Blood donation: knowledge and attitudes of a university population in Chile. Rev Panam Salud Publica 22: 323-238
- City Government of Addis Ababa health bureau annual report 2012.
- Addis Ababa city administration health bureau health institution data base 2014.
- Sabu KM, Remya A, Binu VS, Vivek R (2011) Knowledge, attitude and practice on blood donation among health science students in a university campus, south India. Online journal health allied SCS 10: 6-12
- Rathod GB, Parmar P (2012) Comparison regarding knowledge, attitude and practice of blood donation between health professionals and general population. IJCRR 4: 114-120
- Nwabueze SA, Nnebue CC, Azuike CA, Ezenyeaku, Aniagboso CC et al. (2014) Perception of blood donation among medical and pharmaceutical science students of Namdi Azikiwe University, Awka. Open Journal of Preventive Medicine 4: 515-522
- Misje AH, Bosnes V, Heier HE (2010) Gender differences in presentation rates, deferrals and return behaviour among Norwegian blood donors. Vox Sang 98: 241-248
- Prados MD, María Dolores Fernández H, Dalmiro Prados J, Sonsoles Gómez G, Rita Robles C (2014). Women as whole blood donors: offers, donations and deferrals in the province of Huelva, south-western Spain. Blood Transfus. Jan 12: 11-20
Relevant Topics
- Child Health Education
- Construction Safety
- Dental Health Education
- Holistic Health Education
- Industrial Hygiene
- Nursing Health Education
- Occupational and Environmental Medicine
- Occupational Dermatitis
- Occupational Disorders
- Occupational Exposures
- Occupational Medicine
- Occupational Physical Therapy
- Occupational Rehabilitation
- Occupational Standards
- Occupational Therapist Practice
- Occupational Therapy
- Occupational Therapy Devices & Market Analysis
- Occupational Toxicology
- Oral Health Education
- Paediatric Occupational Therapy
- Perinatal Mental Health
- Pleural Mesothelioma
- Recreation Therapy
- Sensory Integration Therapy
- Workplace Safety & Stress
- Workplace Safety Culture
Recommended Journals
Article Tools
Article Usage
- Total views: 26413
- [From(publication date):
August-2015 - Aug 01, 2025] - Breakdown by view type
- HTML page views : 20214
- PDF downloads : 6199