Risky Sexual Behavior and Associated Factors among Reproductive Age Group High School Students: Institution Based Cross Sectional Study
Received: 18-May-2018 / Accepted Date: 24-May-2018 / Published Date: 31-May-2018 DOI: 10.4172/2161-1165.1000344
Abstract
Background: Young people are the back bone of every counter’s future. At the same time, they are the ones that are at greater risk for many risky sexual behaviors. In Ethiopia, despite the significance of the problem, there is little research work in the area of risky sexual behaviors and associated factors among high school students. The objective of this study was to assess risky sexual behaviors and associated factors in high school students in Shashemene and Bulchana Preparatory Schools.
Methods: A cross sectional study was conducted from April 28-30 E.C. The calculated sample size was allocated to each grade by using simple random sampling technique. A total of 372 students were enrolled in this study. Data were entered using Epi-Data version 3.1 and exported to SPSS version 20 for analysis. Binary logistic regression analysis was used to see significance of association between the outcome and independent variables. Odds ratios at 95% CI were computed to measure the strength of the association between the outcome and the explanatory variables. P-value ˂0.05 was considered as a statistically significant.
Results: From the 372 students participated in the study, 111(29.8%) had sexual experience out of which 72 (64.8%) committed their first sex at less than 18 years of age. The mean age at the first sexual intercourse was 17.04 ± 1.7562.
Being alcohol consumer (AOR: (17.8, 95% CI: (4.23, 75.1), chewing khat (15.41, 95% CI: (2.96, 60.68), whose family do not know where they spent their time (0.027, 95% CI: (0.007, 0.111) and discussion with family about HIV and STI (AOR: (0.006, 95% CI: (0.001, 0.029) were factors significantly associated with risky sexual behavior.
Conclusions: Majority of the students had at least one of the risky sexual behaviors. Alcohol consumption, chewing khat, parental relationship and discussion with family about HIV and STI were factors significantly associated with risky sexual behavior. School Health education on risky sexual behavior should be given to the students. Health bureau, schools, parents and other concerned bodies should give due attention for risky sexual behavior.
Keywords: Risky sexual behavior; Reproductive age; Adolescence
Abbreviations
AOR: Adjusted odd ratio; AIDS: Acquired Immuno Deficiency Syndrome; CI: Confidence Interval; EDHS: Ethiopian Demographic and Health Surveys; HIV: Human immune deficiency virus; SPSS: Statistical Package for Social Sciences; STI: Sexually Transmitted infection; WHO: World Health Organization
Background
Adolescence is the time of transition from childhood to adulthood during which young people experience changes following puberty [1]. Being young mean when one’s appearance is full of freshness vigor and young spirit that distinguish him from other generation. Such characteristic include, desire for independence, zealousness, radicalism, rebellions, curiosity, influenced by friends etc. It is a period of opportunity as well as a time of vulnerability and also a time of experimentation with new ideas which make them vulnerable to health risk and unsafe reproductive health outcomes [2].
This risky Sexual behaviors place adolescent at risk for infection, unintended pregnancy, abortion, Human Immune Deficiency Virus/ Acquired Immunodeficiency Syndrome (HIV/AIDS) and other sexually transmitted infections [3]. Risky sexual activities among adolescents have been reported to be increasing globally. Worldwide age of menarche and in some countries age of first inter course is declining. Studies suggested that age of sexual debut is as low as 9-13yrs for boys and 11-14 yrs for girls. In number of developing countries both genders are increasingly victims of sexual exploitation and much sexual activity during adolescence is coerced, not consensus [4].
In many developing countries, adolescents have become increasingly prone to engage in habitual risky sexual behaviors such as early sexual initiation and unprotected sex. Quantitative and qualitative studies of the sexual knowledge and practices of adolescents reveal that a substantial number of girls and boys in many developing countries engage in sexual intercourse before their 15th birth days. Early and unprotected sexual initiation can trigger a succession of harmful physical, emotional and social outcomes, especially for girls. Moreover, compared with adults, adolescents are less likely to have the foresight, skills, cognitive maturity, information and support they need to protect themselves from unwanted pregnancy, HIV and STIs so are more at risk from this behaviors [5]. There for to reducing sexual risky behaviors and related health problems among youth, schools and other youth serving organizations can help young people adapt lifelong attitudes and behaviors that support their health and wellbeing including behaviors that reduce their risk for HIV, other STDs and unintended pregnancies [6].
Studies in sub-Saharan Africa have also documented high and increasing pre-marital sexual intercourse among adolescents. Especially in developing countries and particularly in Ethiopia, studies have shown that 60% of adolescents’ pregnancy is unwanted [1]. According to the family planning guidance association of Ethiopia, about 72% of boys and 71% of girls have had their first sexual contact within the age range of 15-17 yrs while 13% of them started sexual activity between 10 and 14 yrs of age (8). According to one national finding, the prevalence of premarital sex among high school adolescent students is 19% [1]. Major predisposing factors for increment of sexual activity among adolescents are fall in menarche age, increased premarital sex, deterioration of traditional norms and values that discourage premarital sex, media that transmit new ideas through movies and music and different books that influences adolescents’ attitudes and behaviors worldwide [7].
Even though there were studies done on risky sexual behavior around the world, no study had been done in the study area. Moreover, the magnitude of the problem still need more work among reproductive age group of high school students. Therefore, this study was aimed at assessing the level of risky sexual behavior and associated factors among reproductive age group of high school students. The findings of the study will also use as base line data to bring better future.
Methods
Study area
Shashemene is a town and a separate Woreda in West Arsi Zone, Oromia Region, Ethiopia. The town lies about 150 miles (250 km) from the capital of Addis Ababa. It has latitude of 7°12' north and a longitude of 38°36' east. Except for the eastern portion, the altitude of this Woreda ranges from 1500 to 2300 meters above sea level; Mount Abaro is the highest point. The total area of Shashemene town is 12917 km2 which is represented by its own map. It holds total population of 236544. Among those 118828 are males and 117716 are females. In the town there are 8 sub cities and 33 sector administrations. Shashemene is bordered on the south by the Southern Nations, Nationalities and Peoples Region, on the west by Shala, on the north by Arsi Negele, on the east by the Kore, and on the southeast by Kofele. There are more than 18 Ethiopian ethnic groups live in Shashemene town. Such as Oromo, Amhara, Gurage, Wolayta, Sidama, Hadiya etc. Around 12 foreign ethnic groups are also live in the town. Among them Babishoto, Rasta are among the dominant. The religions found in the town are Muslims, orthodox, protestant, catholic, waaqeffata and Adventist and most people use Afan Oromo for communication. There are 10 secondary and 5 preparatory schools in the town including both the government and private ones.
Study design and period
Institutional based cross-sectional study was conducted from April to May, 2015.
Study participants
The source population of the study was all reproductive age group students of secondary and preparatory schools in Shashemene town. The study population was reproductive age group students who learn in two of the government preparatory schools. All students in age group of 14-19 who were learning in shashemene and Bulchana preparatory school were included in the study. Those physically and mentally unable to respond and those Severely ill students and students who are dropped out from the school in the mid-year were excluded from the study.
Sample size determination and sampling technique
The sample size was estimated using sample size determination formula a prevalence level that estimate maximum sample size (53.3% from similar studies), marginal error (d) 0.05, non-response rate of 0.1, with 95 percent confidence certainty and alpha 0.05, the determined final sample size, by using the correction formula, was 372.
Students in the schools were stratified by their grade in the two selected preparatory schools. List of students of grade 11 and 12 was prepared and used as a sampling frame. Sample size was allocated for every strata based on proportional allocation to their size. Finally students from every class were selected by simple random sampling (Figure 1).
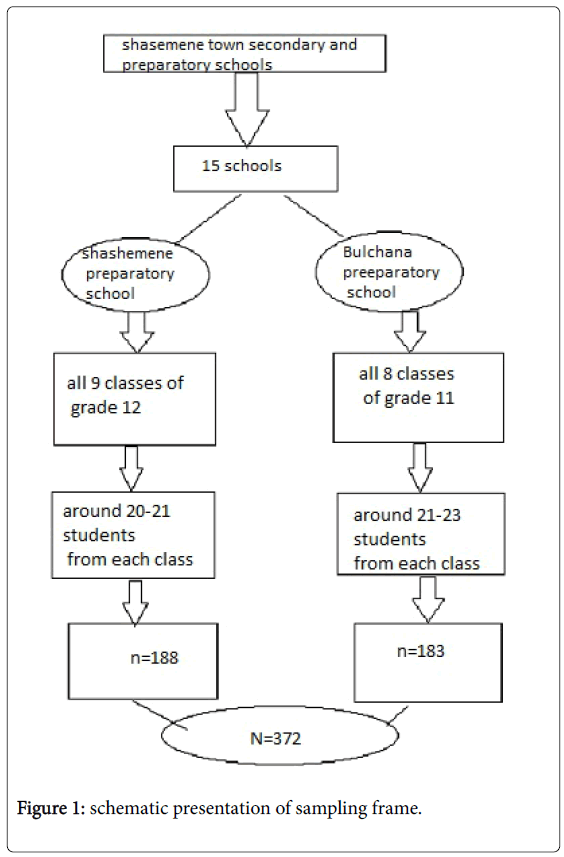
Figure 1: schematic presentation of sampling frame.
Data collection
Structured and pretested questionnaire was used to collect from each study subject. The questionnaire was adapted after review of relevant literatures. The questions and statements was grouped and arranged according to the particular objective that they can address. The questionnaires consist of three parts. Part I consists of sociodemographic characteristics. Part II contains questionnaire that would assess sexual history; number and type of partners and Part III contains about substance abuse. Three diploma nurses were recruited as data collectors and two public health degree as supervisor.
Quality assurance
Training of data collectors and supervisors was made for 2 days to enable them acquire basic skills necessary for data collection and supervision, respectively. Pre-testing of data collection tool was made in schools other than the study area on 5% of sample. Based on the results of pre-testing, data collectors were reoriented and the questionnaire was modified as necessary. The principal investigators and supervisors made a day to day on site supervision during the whole period of data collection. Completeness of the information on all variables and legibility of each filled in the questionnaire/check list was audited at the end of each day to ensure accuracy.
Data analysis
Data were entered and cleaned using Epi-Data version 3.1 and exported to SPSS version 16 for analysis. Descriptive statistics (Frequency, mean, standard deviation, and proportion) was calculated to summarize the findings. Results were presented by tables. Binary logistic regression was used to predict variables which have independent association with outcome variable. Variables which have a significant association at p-value <0.05 in the bivariate analysis were taken to multivariate analysis to include all potential variables. Odds ratio at 95% CI was used to check for the existence and strength of association between independent and outcome variables. P-value of less than 0.05 was considered as statistical significant in the multivariate analysis.
Results
A total of 372 students participated in the study with 100% response rate. Among the participants, 199(53.5%) were males and the majority, 262(70.5%) were in the age group 18-19 years. Concerning ethnicity, Oromo was the dominating ethnic group 232(62.4%), followed by Amhara 72(19.4%). Orthodox Christianity, was dominant religion accounting for 168(45.2%) followed by Islam 117(31.5). From the total students included in this study, 346(93.0%) attend their primary school in urban. Regarding marital status, the majority of students, 363(97.6%) was single. concerning the living arrangement, 267(71.8%) were living with their parents. Among the total 372 respondents 268(72.0%) students’ parents know their daily activity and the rest clam their parents have no idea where they been. Regarding discussion with their parents, 261(70.16%) of them didn’t talk about the transmission ways of STI and HIV/AIDS.
From the total of 372 students, for 174(46.9%) the average monthly income of their family was 500-1500. 236 (63.6%) of the respondents earn money. From those who got money 137 (58.3%) got ≤ 100 birr monthly. From those students who got money 76 (32.5%) spend it for buying books (Table 1).
| Variables | Total (N and %), N=372 |
|---|---|
| Sex | |
| Male | 199(53.5%) |
| Female | 173(46.5%) |
| Age | |
| 16-17 | 110(29.5%) |
| 18-19 | 262(70.5%) |
| Ethnicity | |
| Oromo | 232(62.4%) |
| Amhara | 72(19.4%) |
| Gurage | 39(10.5%) |
| Wolayta | 12(3.2%) |
| Sidama | 7(1.9%) |
| Others | 10(2.7%) |
| Religion | |
| Orthodox | 168(45.2%) |
| Muslim | 117(31.5%) |
| Protestant | 77(20.7%) |
| Catholic | 8(2.2%) |
| Others | 2(0.2%) |
| Grade | |
| 11th | 183(49.2%) |
| 12th | 189(50.8%) |
| Attending primary school | |
| Urban | 346(93.0%) |
| Rural | 26(7.0%) |
| marital status | |
| Single | 363(97.6%) |
| Married | 9(2.4%) |
| living with | |
| Mother/father | 267(71.8%) |
| Brother/sister | 36(9.7%) |
| Mother only | 28(7.5%) |
| Grand parents | 18(4.8%) |
| Father only | 4(1.1%) |
| Others | 19(5.1%) |
Table 1: Socio-demographic characteristics of shashemene preparatory school, shashemene town, west Arsi zone, Oromia, Ethiopia in 2015.
Level of Risky Sexual Behaviors
From 372 respondents, 337(90.6%) had knowledge about HIV and sexually transmitted diseases. From students who were reported having knowledge about HIV and STIs, 246(66.1%) got the information from mass media like radio, TV and newspaper. Among the respondents, 262(69.4%) never had sex and the rest 111(29.8%) had sex. From the total participants who had sex 104(27.9%) of them had premarital sex, and from those who had premarital sex 80(76.9%) of them were males and 24(23.1%) of them were female. vaginal sex was the commonest type of sex mostly practiced 110(99.9%). From those who had sex the majority 72(64.8%) started having sex before age of 18, out of which 43(59.7%) of them were male. The mean age at first sexual intercourse was 17.04 ± 1.75. From 111 students who had sexual experience 60(54.1%) used condom regularly. From the respondents who had sex, 62(55.9%) of them had sex with more than one person. And from 81 male students who had sex 19(17.1%) of them had sexual intercourse with commercial sex workers. With regarding to test for those who had sex the majority of the students 99(95.2%) were tested for HIV and from those 10(18.9%) of them were positive and from those who wear positive 7 of them started ART and the rest of 3 students didn’t took any measures. 11 of them were tested for pregnancy and 5 of them was pregnant and from those who were pregnant 2 of them did abortion in health institute, 2 of them did abortion in traditional places and one of them gave birth. 4 of them were tested for STI only and one of them was positive and get treatment (Table 2).
| Variables | Total (N and %), N =372 |
|---|---|
| Knowledge | |
| Knowledgeable | 337(90.6%) |
| Not knowledgeable | 35(9.4%) |
| Source of information(n=337) | |
| Mass media | 203(60.2%) |
| Health professionals | 70(20.8%) |
| Teachers | 28(8.3%) |
| Family | 24(7.1%) |
| Friends | 9(2.7%) |
| Library | 3(0.9%) |
| Had sex | |
| No | 262(69.4%) |
| Yes | 111(30.6%) |
| Type of sex(111)* | |
| vaginal sex | 110(99.9%) |
| Oral sex | 11(9.9%) |
| Anal sex | 10(9.0%) |
| Condom use (111) | |
| No | 51(45.9%) |
| Yes | 60(54.1%) |
| No of sexual partners | |
| One | 62(55.9%) |
| More than one | 49(44.1%) |
Table 2: Risky sexual behavior among shashemene preparatory school, shashemene town, west Arsi zone, Oromia, Ethiopia in 2015.
Substance abuse
Among 372 students who participated in the study, 126(33.8%) of them consume alcohol, 79(62.7%) of them being male students. Regarding the frequency from the total consumers, 60(47.3%) of them consumed alcohol 2 times per week, 37(29.7%) of them consume it more than 3 times within a week and the rest of 29(23.0%) students consume it only ones a week. And majority of students 55(43.2%) had sexual intercourse after they drink alcohol and from those who had sex after consumption 31(56.25%) of them had sex occasionally 24(43.75%) of them practices it usually, and the rest 23(28.4%) of them did reading, 12(14.8%) of them fight, 10(12.3%) of them sleep and 1 (1.2%) perform other things like walking and going to night cubs after they consume alcohol. 132(32.5%) students chew khat, from those 75(57.4%) of them started it 1 year back 50(38.3%) of them started it this year and the rest of 6(4.3%) students gave response for this question and regarding the frequency 73(55.3%) students chew it two times per week, 33(25.5%) chew it three times per week and 25(19.1%) chew it once per week. 33(8.8%) respondents reported that they smoke cigarette, regarding amount 18(54.5%) of them smoke more than 3 cigarette per day, 12(36.4%) smoke two cigarette per day, 3 (9.1%) smoke one cigarette per day, From those smokers 15 (45.5%) of them started it 1 years back, 15(45.5%) of them started it this year and the rest of the students 3(9.1%) didn’t remember when they started smoking. 24(31.3%) of them used drugs like marijuana and shisha. From 24(6.4%) students who used drugs 14(58.3%) of them used marijuana and 10(41.7%) of them used shisha. The major pushing factor for those students who used drugs and alcohol were peer pressure 80(52.4%), for enjoyment 54(35.4%), due to depression 11(7.3%), 4(2.5%) didn’t have reason and the remaining 4(2.5%) used because their family consume it.
Factors associated with risky sexual behavior
Result of bivariate analysis showed that age (p<0.005), sex (p<0.001), marital status (p<0.005), family Know student daily activity (p=0.010) Discussion with family about HIV and STIs (p=0.010), alcohol drinking (p<0.001), Chewing Khat (p<0.001) and cigarette smoking (p<0.001) were identified as candidates for multivariate analysis at p-value <0.05 (Table 3).
| Risky sexual behavior N (%) | Crude Odds ratio at 95%CI | Adjusted Odds ratio at 95%C | ||
|---|---|---|---|---|
| Variables | No | Yes | ||
| Age | ||||
| 16 | 2(0.5 ) | 8(2.1) | 0.329(0.066-1.639) | 0.224(0.038-1.31) |
| 17 | 17(4.5) | 83(22.3) | 0.269(0.138-0.527) | 0.209(0.082-0.53) |
| 18 | 48(12.9) | 126(33.8) | 0.501(0.293-0.858) | 0.43(0.218-0.86) |
| 19 | 38(10.2) | 50(13.4) | 1 | 1 |
| Sex | ||||
| Male | 75(20.1) | 124(33.3) | 2.88(1.772-4.692) | 2.507(1.37-4.56) |
| Female | 30(8.1) | 143(38.4) | 0.1 | 1 |
| Family know student daily activity | ||||
| Yes | 57(15.3) | 206(55.4) | 2.891(1.790-4.671) | 0.27(0.007-0.111) |
| No | 48(12.9) | 60(16.1) | 1 | 1 |
| Discuses about HIV &STIs | ||||
| Yes | 17(4.6) | 93(25) | 2.783(1.56 2-4.956) | 0.006(0.001-0.029) |
| No | 88(23.6) | 173(46.5) | 1 | 1 |
| Alcohol drinking | ||||
| Yes | 41(11.0) | 33(8.9) | 0.220(0.129-0.376) | 17.81(4.225-75.09) |
| No | 64((17.2) | 234(62.9) | 1 | 1 |
| Chewing Khat | ||||
| Yes | 24(6.4) | 23(6.1) | 3.143(1.683-5.871) | 13.40(2.962-60.67)* |
| No | 81(21.7) | 244(65.6) | 1 | 1 |
| Cigarette smoking | ||||
| Yes | 22(5.9) | 11(2.9) | 6.169(2.871-13.25) | 3.81(0.71-20.50) |
| No | 83(22.3) | 256(68.8) | 1 | 1 |
Table 3: Factors associated with risky sexual behavior among shashemene town preparatory students, 2015.
Age, sex, marital status, family Know student daily activity, discussion with family about HIV &STIs, alcohol drinking, Chewing Khat and cigarette smoking were significantly associated with risky sexual behavior (Table 3).
Risky sexual behavior was 79% less likely among students whose age was17 year as compared to those with age 19 years (AOR: 0.209, 95%CI: (0.082-0.53)) and students whose age was 18 years were 57% less likely to had risky sexual behavior as compared to those with age 19 (AOR: 0.430, 95%CI: (0.218-0.860)).
Males had 2.5 times more odds of risky sexual behavior as compared to female students (AOR: 2.507, 95%CI: (1.370-4.560)).
Students who consumed alcohol had 17 times more odds of risky sexual behavior than non-alcohol consumers (AOR: 17.81, 95%CI: (4.225-75.093)).
Those who chew Khat had 13 times more odds of risky sexual behavior than those who did not chew Khat (AOR: 15.406, 95%CI: (2.962-60.678)). The odds of risky sexual behavior of the student’s family who did not know where they spent their time is higher by 73% among the corresponding students (AOR: 0.027, 95%CI: (0.007-0.111)). The students who had discussed with their family; about HIV and STI had higher odds of risky sexual behavior (AOR: 0.006, 95%CI: (0.001-0.029)).
Discussion
According to this study, 29.8% of the participants had sex and from which 23% had risky sexual behaviors. The findings showed almost the same prevalence in aspect of number of participants who have sex with study done in Boditti, Ethiopia which was 29.1%. But, lower prevalence of risky sexual behaviors when we compare this to study conducted in Boditti which was 61.5% [8]. The low prevalence may be due to rising awareness and easily accessibility of health information.
In this study, about 99.9% had vaginal sex, 9.0% and 9.8% had reported to have oral and anal sex respectively. In the study done in Boditti town oral sex was 5.1% and anal sex was 1.3% [8]. This showed that high prevalence of oral and anal sex in Sashemene preparatory school. This might be because of Shashemene is a big town and students had access to pornographic films and internet access and also the time gap may be the reason.
The prevalence of premarital sex was 23.1% in this study. But, the national finding of the prevalence of premarital sex among high school adolescents was 19%. And in other study conducted in Nekemt high school adolescent’s premarital sex were 21.5% [1] and also in other study conducted in Boditti was 22.2% [8]. This shows that our finding was higher than the three data’s this may be due to town difference that means since shashemene town is a big city and also it may be due to the time differences between the researches.
In our study 45.9% of the students didn’t use condom this shows almost comparable result with Agaro which was 45.6% [9]. But lower result when compared to study conducted in Boditti which was 67.6% [8]. Also in this study the number of respondents who didn’t use condom during the last sexual intercourse was 42.3%. This verifies that it had low prevalence when compared with the study conducted in Nekemt high school, which was 67.1% [1]. This low prevalence might be because of time variation, neglecting the disaster of HIV/STI and increasing prevalence of drug and alcohol consumption.
In our study 55.9% have more than one sexual partner when we compare this to study conducted in Gonder which was 53.3% [10] but lower than the study done in Boditti which was 70.3% [9]. The high prevalence when compared to Boditii may be due to increasing learning Medias which teaches about the risk of having more than one partner and it may also be due to cultural change with time.
In our study 17.1% had sex with commercial sex workers. In contrary, study conducted in Humara, Ethiopia showed that 38% of students had sex with commercial sex workers [11]. This may be due to increasing awareness about communicable disease and it may be due to increasing man and women romantic relationship.
Among the study participants 33.8% AOR 17.81(4.225-75.09) of them consume alcohol, 32.5% AOR 13.40(2.962-60.67 chaw chat and 8.8% smoke cigarette, when we compare this study with the study conducted on Humera which was 74.15% consume alcohol, 37.9% chaw chat and 6.3% smoke cigarette [11]. This shows low prevalence of alcohol and khat but high prevalence of cigarette, this low prevalence may be due to the living arrangement and cultural and religious difference but the high prevalence in cigarette may also be due to cultural variation and presumed modernization. In our study students whose parents didn’t know where they been was 38% this shows high magnitude when compared to national findings. This may be due to increasing work hour and globalization.
Limitation of the Study
Since our study deals with a very personal and sensitive issue- which was about risky sexual behaviors, obtaining an honest response among adolescents is difficult. Hence, some sort of desirability bias may not be eliminated, even if we have tried our best to minimize it.
Conclusion
In our study majority of the students have knowledge about STI/HIV/AIDS but it turn out large amount of the participants have risky sexual behaviors like having multiple sexual partners, practicing early sex, not using condom and also having sex with commercial sex workers.
Alcohol consumption, chewing khat, parental relationship and discussion with family about HIV and STI were factors significantly associated with risky sexual behavior. Therefore, School Health education on risky sexual behavior should be given to the students and Health bureau, schools, parents and other concerned bodies should give due attention for risky sexual behavior.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from Institutional Review Board of Hawassa University College of medicine and health science. Permission letter was obtained from Shashemene town education bureau. Other concerned bodies of the schools were also informed about the study. All the information retrieved was kept in the way that could not interfere in personal confidentiality. Informed consent was obtained from each study participant after explanation of the purpose of the study. All sample populations were encouraged to participate in the study while at the same time they were told their right not to participate.
Availability of Data and Materials
The datasets during the current study are available from the corresponding author on reasonable request.
Acknowledgements
We would also like to extend our sincere appreciation to Hawassa University, College of Medicine and Health Science, School of Public and Environmental Health for giving us this golden opportunity to conduct this research. We would also like to thank shashemene town education bureau for providing relevant information for this research activity. Lastly, we would like to thank shashemene preparatory school staffs and students for their cooperation.
Authors’ Contributions
HS conceived the research idea, conducted the data collection, data analysis and data interpretation, and wrote and reviewed the paper. TY conducted the data analysis, data interpretation, and wrote and reviewed the paper. Both authors read and approved the final paper.
References
- Seme A, Wirtu D (2008) Premarital sexual practice among & school adolescents in Nekemt town, East Wollega, Ethiopia. Ethiop J Health Dev 22: 167-172.
- Mercy ON, Peter AS (2014) Risky sexual behavior among female high school students in Nigeria. European Scientific Journal l0: 31.
- Tewabe Y (2009) Education, HIV/AIDS, and Sexual Reproductive Health: Exploring the Unmet Information Needs of Young people: The case of Addis Ababa and Bahir Dar, Ethiopia. Addis ababa.
- World Health Organization (2003) WHO information series on school health. World Health Organization, Geneva.
- Yi S, Poudel KC, Yasuoka J, Palmer PH, Yi S, et al. (2010) Role of risk and protective factors in risky sexual behaviour among high school students in Cambodia. BMC public health 10: 1471-2458.
- Education Development Center (2009) Introduction to risky sexual behavior. EDC Program.
- EPHI (2004) Module on adolescent reproductive health. Mekelle University, carter center (EPHI) and FDRE Ministry of Education and MOH.
- Daka D, Shaweno D (2014) Magnitude of risky sexual behavior among high school adolescents in Ethiopia: A cross-sectional study. J Public Health Epidemiol 6: 211-215.
- Girma B, Assefa D, Tushunie K (2004) Determineants of condom use among Agaro high school students using behavioural models. Ethiop J Health Dev 18: 25-30.
- Kitaw Y, Worku A (2002) High risk sexual behavior and pattern of condom utilization of Gondor College of Medical Science (GCMS) Students, Ethiop J Health Dev 16: 335-338.
- Fekadu A, Gebrethadkan J (2014) Risky sexual behavior and associated factors among humera secondary students. Ethiopia Journal of Public Health 2: 410-416.
Citation: Seyfu H, Yohannes T (2018) Risky Sexual Behavior and Associated Factors among Reproductive Age Group High School Students: Institution Based Cross Sectional Study. Epidemiology (Sunnyvale) 8: 344. DOI: 10.4172/2161-1165.1000344
Copyright: © 2018 Seyfu H, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Select your language of interest to view the total content in your interested language
Share This Article
Recommended Journals
Open Access Journals
Article Tools
Article Usage
- Total views: 6347
- [From(publication date): 0-2018 - Dec 09, 2025]
- Breakdown by view type
- HTML page views: 5298
- PDF downloads: 1049