A Retrospective Pilot Study: The Efficacy of Serratus Anterior Plane Nerve Catheters as an Alternative to Thoracic Epidural Catheters in the Treatment of Pain for Thoracic Surgeries
Received: 11-Sep-2018 / Accepted Date: 25-Sep-2018 / Published Date: 01-Oct-2018
Abstract
Background and objectives: The serratus anterior plane block is a regional anesthetic technique performed under ultrasound guidance that can provide analgesia to the thoracic wall as an alternative to the thoracic epidural. We hypothesize that the use of the Serratus Anterior Plane Block (SAPB) would provide non-inferior pain control with fewer episodes of hypotension requiring pharmacologic management, when compared with thoracic epidural analgesia.
Methods: The study population includes patients, who were above the age of 18, were ASA 2-3, who underwent thoracotomy surgeries between 7/1/2014 to 7/1/2017. The primary outcomes being measured are notable episodes of hypotension, requiring pharmacologic vasopressor management, adjustments in the epidural block doses, and the need to discontinue the epidural. Serial trends in MAP, HR, and BP were collected and presented for the entire cohort in the first 24 hours. Secondary outcomes were measured as total morphine equivalents as well as median pain scores during the first 24 hours.
Result: At our institution, a retrospective chart review of serratus plane nerve blocks revealed a total of five performed in the setting of a thoracotomy. When compared to thoracic epidurals, notable episodes of hypotension, morphine equivalents, and the visual analog scale were measured compared to the SAPB.
Conclusion: The SAPB appear to be a safe alternative method to treating postoperative acute thoracotomy pain in the presence of any contraindications to thoracic epidural analgesia.
Keywords: Thoracic epidural; Analgesia; Hypotension; Serratus anterior plane block (SAPB)
Introduction
Thoracotomies are notoriously painful in the acute post-operative setting [1]. The gold standard for pain control for the patient who undergoes open thoracic surgery is the placement of a thoracic epidural catheter (TEC) [2,3]. While thoracic epidural placement provides the most reliable pain control in the intraoperative and postoperative phase, it may be contraindicated in patients with hemodynamic instability or those with thrombocytopenia [4]. With the use of an ultrasound-guided regional anesthetic block technique, the serratus anterior plane block (SAPB) provides analgesia to the thorax by depositing local anesthetic above or below the serratus anterior muscle [5,6]. The lateral cutaneous branches of the intercostal nerves are blocked before they divide into the anterior and posterior branches with analgesia typically provided from thoracic levels T2 through T9 [7]. The purpose of this study is to provide clinical evidence that the SAPB is non-inferior to the thoracic epidural in the setting of a thoracotomy.
Methods
Data for this study was provided by the Arkansas Clinical Data Repository (AR-CDR) maintained by the Department of Biomedical Informatics in the College of Medicine at the University of Arkansas for Medical Sciences (UAMS). The AR-CDR is approved to operate as an enterprise data resource to support research across UAMS. Data in the AR-CDR comes from UAMS Electronic Medical Record (EMR), tumor registry, billing, and cancer genomic data and comprises encounters since 05/01/2014.
Patients were placed in supine position with their arm abducted over their head. Using linear ultrasound, the probe was placed over the fifth rib in the mid axillary line and using an in place technique to visualize the echogenic needle. The needle was advanced to pierce the inter-fascial plane between the serratus anterior muscle and the fifth rib (Figure 1). Hydro-dissection was performed with 5 ml of normal saline followed by 20 ml of 0.25% bupivacaine. The catheter was advanced into the space created and secured with mastisol, steri-strips, and tegederm tape. The On-Q medicine ball was attached to the catheter at a constant rate of 14 mL/hr with a concentration of 0.25% bupivacaine being administered continuously.
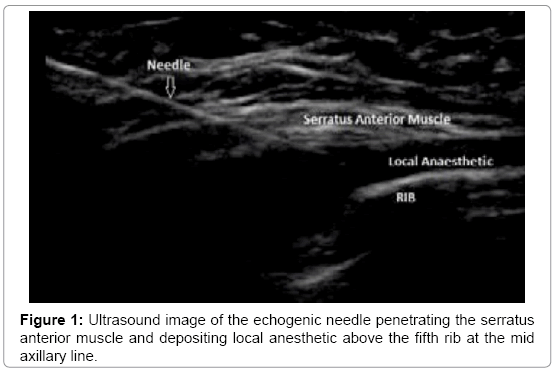
Figure 1: Ultrasound image of the echogenic needle penetrating the serratus anterior muscle and depositing local anesthetic above the fifth rib at the mid axillary line.
Result
Of the five patients who received the SAPB, there were zero cases of hypotension during the first 24 hours of postoperative hospital stay. As seen in Table 1, 77% of patients developed hypotension defined as a decrease in systolic blood pressure greater than 20% from baseline. In Table 2, A Chi-squared analysis was used for measuring the primary outcome data, and the T-test was conducted for analysis of morphine equivalents. Comparison of supplemental IV and PO pain medicine was converted to morphine equivalents for standardization. Of the two groups, the SAPB group consumed twice as much opioids, 86.5 ± 3.5 while the TEC group consumed an average of 40 ± 4.1 morphine equivalents. The visual analog score was also a measured secondary outcome among the TEC and SAPB group, using the Mann-Whitney U test we deduced that the SAPB group had a median VAS score of 7, whereas the TEC group’s VAS score was 4.5. The results of this study were not statistically significant as the p value was 0.02. Major limitations of this study include a low power, since this retrospective chart review identified only five patients who received a SAPB. This newer ultrasound guided block for analgesia is currently limited secondary to lack of popularity of this new peripheral nerve block.
| Test 1 | TEC | SAPB |
|---|---|---|
| ASA 2 | 6 | 1 |
| ASA 3 | 28 | 5 |
| Age (years) | 61 ± 21 | 60.2 ± 23.4 |
| Female (%) | 38% | 33% |
Table 1: Determine efficacy of Serratus Anterior Plane Nerve Catheters (SAPB) as an alternative to Thoracic Epidural Catheters (TEC) in the treatment of pain for thoracic surgeries.
| Test 2 | TEC | SAPB | p-value |
|---|---|---|---|
| Hypotension | 77% (60.7, 88.2) | 0% (0, 48) | 0.0006 |
| Morphine equivalents | 40 ± 4.1 | 86.5 ± 3.5 | <0.0001 |
| VAS | 4.5 [3,6] | 7 [5,8] | 0.02 |
Table 2: Analysis of hypotension, morphine equivalent and VAS (Visual Analog Score) among TEC and SAPB group.
Discussion and Conclusion
The Serratus Anterior Plane Nerve Block is a safe alternative to treating postoperative acute thoracotomy pain in the setting of any contraindications to thoracic epidural analgesia. While the TEC is superior, the SAPB provides comparable analgesia without the adversity of hypotension. This novel technique has been used for thoracotomies, thoracoscopies, rib fractures, breast surgery, and shoulder surgery. With stable hemodynamics and comparable pain scores in the early postoperative period, the Serratus Anterior Plane Nerve Block is another technique that can be combined to develop a multimodal approach to analgesia.
Acknowledgements
Dr. Jill Mhyre, chairperson of the University of Arkansas for Medical Sciences has given her time and assistance to better statistically analyze this study.
References
- Kavangh BP, Katz J, Sandler AN (1994) Pain control after thoracic surgery: A review of current techniques. Anesth 81: 737-759.
- Mesbah A, Yeung J, Gao F (2016) Pain after thoracotomy. Â BJA Educ 16: 1-7.
- Block BM, Liu SS, Rowlingson AJ, Cowan AR, Cowan JA Jr, et al. (2003) Efficacy of postoperative epidural analgesia: A meta-analysis. JAMA 290: 2455-2463.
- Khalil AE, Abdallah NM, Bashandy GM, Kaddah TA (2017) Ultrasound-guided serratus anterior plane block versus thoracic epidural analgesia for thoracotomy pain. J Cardiothorac Vasc Anesth 3: 152-158.
- Blanco R, Parras T, McDonnell JG, Prats-Galino A (2013) Serratus plane block: A novel ultrasound-guided thoracic wall nerve block. Anesthesia 68: 1107-1113
- Nagdev A, Mantuani D, Durant E, Herring A (2017) The ultrasound-guided serratus anterior plane block. ACEP Now 36: 12-13.
- Sentürk M, Ozcan PE, Talu GK, Kiyan E, Camci E, et al. (2002) The effects of three different analgesia techniques on long-term postthoracotomy pain. Anesth Analg 94: 11-15.
Citation: Suvar T, Shah A, Crabtree D, Mhyre J (2018) A Retrospective Pilot Study: The Efficacy of Serratus Anterior Plane Nerve Catheters as an Alternative to Thoracic Epidural Catheters in the Treatment of Pain for Thoracic Surgeries. Anesth Commun 2: 103.
Copyright: © 2018 Suvar T, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Select your language of interest to view the total content in your interested language
Share This Article
Open Access Journals
Article Usage
- Total views: 3574
- [From(publication date): 0-2018 - Dec 21, 2025]
- Breakdown by view type
- HTML page views: 2651
- PDF downloads: 923