Research Article Open Access
Influence of Vascular Occlusion in Concentration of Growth Hormone and Lactate in Athletes during Strengthening Quadriceps Exercise
Saulo Nani Leite1, Amir Curcio Dos Reis2*, Gustavo Lacreta Toledo Colnezi2, Fernando Henrique Amorim Souza3, Haroldo Fernando Silva Ferracini3, Paulo Roberto Garcia Lucareli2 and Samuel Straceri Lodovichi2
1Associate Professor and Staff Physical Therapist, Irmandade da Santa Casa de Misericordia de São Paulo – ISCMSP, Brazil
2Department os Rehabilitation Science, Human Motion Analysis Laboratory, Universidade Nove de Julho, São Paulo, Brazil
3Physical Therapist, Centro Universitário da Fundação Nacional de Guaxupé – UNIFEG, Guaxupé, MG, Brazil
- *Corresponding Author:
- Amir Curcio dos Reis
Department os Rehabilitation Science
Human Motion Analysis Laboratory
Universidade Nove de Julho, São Paulo,Brazil
Tel: (55+11) 60671234
E-mail: acrfisio@globo.com
Received date: July 16, 2014, Accepted date: March 23, 2015, Published date: March 27, 2015
Citation: Leite SN, Reis ACD, Colnezi GLT, Souza FHA, Ferracini HFS, et al. (2015) Influence of Vascular Occlusion in Concentration of Growth Hormone and Lactate in Athletes during Strengthening Quadriceps Exercise. Occup Med Health Aff 3:195. doi:10.4172/2329-6879.1000195
Copyright: © 2015 Leite SN, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Visit for more related articles at Occupational Medicine & Health Affairs
Abstract
Objective: The aim of this comparative experimental study designed is analyze the possible changes in GH serum and lactate during the performance of resistance exercise-induced ischemia in young athletes. A possible outcome will be to promote greater strength gains and muscle hypertrophy during the training protocol.
Design: This survey was conducted with 18 male football players 18 years of age. The athletes were divided into two groups; one group was subjected only to quadriceps exercises; the other group was subjected to quadriceps exercises associated with vascular occlusion. Levels of lactate and GH were observed before and after resistance exercise.
Results: Comparing intergroup data, there were no statistically significant results. However, when comparing data within the groups, there was an increase in Group 2 obtained for both the lactate threshold and GH. Group 1 showed an increase in the lactate threshold, but a decrease in GH.
Conclusions: This new method of resistance training should be analyzed, and further experiments are needed to optimize the protocol to reach optimum high intensity resistance training in young athletes.
Keywords
Ischemia; Growth hormone; Lactic acid; Resistance training; Therapeutic occlusion
Introduction
Resistance exercise is defined as a type of active exercise in which a dynamic or static muscle contraction is set against an external force. This external force can be applied manually or mechanically [1], which generally causes an increase in muscle size and strength. If the objective is to gain muscle mass, both high and medium intensity exercises must be utilized with a relatively short period of rest between bouts of exercise [2].
During exercise, blood flow is an important factor in the transport of oxygen to the muscle. During sub-maximum exercise, it is important to increase blood flow in order to meet the demand for oxygen and remove waste products from the muscles. Therefore, any type of vascular occlusion will have direct impact on the performance of muscle activity [3].
In recent years, several studies have shown that lower intensity exercise (20-50%) of maximum resistance (MR), combined with resistance training at an appropriate level of compression on the limb can lead to a partial ischemia; this phenomenon has also been observed during high-intensity exercise [4].
Some researchers emphasize that a reduction in muscle blood flow (RMBF) during endurance exercise has been widely used in order to induce the muscle to improve strength and trophism; thus, achieving results similar to those gained with high strength and high intensity training. This exercise regime is viewed as an advantage because lower loads are used during exercise [5].
We know that when dealing with resistance exercises, there is induced ischemia due to dynamic contractions with and without intensity greater than 30% of 1 MR. Of course, there is an increase in intramuscular pressure, which increases linearly with muscle tension and causes capillary collapse, therefore, exacerbating the anaerobic metabolism [6].
The increase in muscle mass during strengthening exercises takes place mainly by hypertrophy of each fiber present in the muscle due to the increasing diameter of filaments and their myofibrils [7].
To improve the response to muscle training, recent studies involving vascular occlusion with high-intensity exercise has shown that this technique can induce biochemical changes favorable to arm and knee flexor extensor muscles in young athletes; this is an important tool in the process of muscle strengthening exercises[8].
The blood concentration in muscle interferes with various chemical factors important in the strengthening process. Lactate, for example, which is a metabolite of anaerobic glucose, alters its concentration level due to exercise intensity. Studies indicate that the lactate threshold (LT) is an invasive gold-standard in determining the anaerobic threshold [9]. This threshold has been widely recommended in the assessment, prescription, and monitoring of exercise programs, especially in cyclical activities like swimming, running, and cycling [10].
Although there are several assumptions about the causes of lactate accumulation during an accelerated non-resistance dynamic exercise test [11], and during resistance exercises, the main factor during the increased production of lactate is muscle hypoxia, because the demand for oxygen decreases due to the collapse of capillaries [6].
In addition to lactate concentration, resistance exercises can also increase concentrations of hormones such as testosterone, growth hormone (GH) and IGF-1. The magnitude of this increase depends on the intensity, volume, rest interval, and number of resistance exercise sessions [12]. GH promotes the growth of organs and is an important regulator of a healthy metabolism and promotes resistance to disease. It is present in most tissues, including muscles, fatty tissue, liver, heart, kidneys, brain, and pancreas [13].
This hormone is produced in the anterior pituitary gland located at the base of the brain and its release is determined by the central nervous system, which in turn controls the demands of the organism as a whole [7]. In the case of the circadian rhythm of GH release, healthy adults present a production of 0.5 mg/day, which is slow and stable, followed by abrupt peak secretions (15-20 mg/l) [14]. However, women demonstrate a more frequent release of GH, both at rest and when under stress, as compared to males [15]. Physiologically, it is only during sleep that men present more GH secretion, and in most cases, this secretion is lower than the secretion observed in women [16].
In the course of human development, GH secretion in both sexes reaches peak concentrations during periods of growth, especially in youth [17]. After this growth period, the secretions remain constant because the amplitude, or the intensity reduces the secretion; it is not difficult to find young people who secrete on a typical day more than double the amount of GH than older individuals [18]. The mechanisms responsible for these changes are not clear in the literature. Nevertheless, many other factors can influence the secretion of GH such as nutrition [19], excess body fat, stress, and level of physical activity, or training [20]. After physical training, GH secretion and reduced blood flow appear to be an important factor in muscle hypertrophy and strength gain in young male athletes.
It is not difficult to find studies in the literature stating that RMBF during resistance training induces hypertrophy and strength gains similar to exercises performed in a traditional manner, with the advantage of having lower intensities [5]. However, there are few studies that document the increase in GH production and changes in lactate threshold exercises associated with vascular occlusion in young athletes. Thus, this study is important in order to ascertain whether there is an increase in these hormones in muscle tissue that can lead to direct tropism benefits.
The aim of this study is to check possible changes in serum GH and lactate associated with induced ischemia in comparison with a control group; and assess serum GH and lactate before and after exercise.
Materials and Methods
Experimental subjects
The survey was conducted with 18 male football players, all participants were 18 years old. An explanation was given to the athletes regarding the techniques that would be applied in the study and that participation in the project was voluntary. Furthermore, the participants signed a Consent form that had been approved by the Research Ethics Committee UNIFEG under Protocol 201.
Standardization of the groups
The athletes were divided randomly into two groups, namely: group 1 (n=9) and underwent only exercise for the quadriceps without occlusion; and group 2 (n=9): performed exercise for the quadriceps associated with vascular occlusion.
Materials
Utilized during the performance of the exercises, was the leg extension, sphygmomanometer, (Sankey ML017/2001®) whose cuff measures 22 inches long and 12 cm wide, from the Physiotherapy Clinic of Maria de Almeida Santos. In order to collect blood, we used cotton, alcohol (70%), sterile and disposable needles, disposable syringes (10 ml), a tourniquet, and a sterile tube without anticoagulants.
Strengthening protocol
The athletes were submitted to a protocol to strengthen the quadriceps muscle for the specific group which formed part of this protocol and consisted of low-intensity exercise at 50% of 1 MR for the participants in group 2 and high-intensity exercise for individuals in group 1, with resistance equivalent to 80% of 1 MR.
Description of the exercise
with their knees flexed at 90°. The exercise was performed isotonically in knee extension, distal resistance was provided by a distal weight, utilizing two sets of 30 repetitions with an interval of 30 seconds between each repetition [2].
In group 2, the athletes were positioned as described above, and the exercise was performed in the same way, with the difference being determined by the vascular occlusion cuff, which was inflated to 100 mmHg, corresponding to an average of 1.3 times the diastolic blood pressure for each individual [2].
Collection and assessment of lactate and GH
Before starting training for muscle strength and following the recommendations of the Brazilian Society of Clinical Pathology and Laboratory Medicine, a qualified nurse collected blood samples from both groups [21]. After 15 minutes post-exercise, a new collect of blood was made in both groups.
The method used for determination of serum GH was by chemiluminescence (Siemens Medical Solutions, Los Angeles, CA, with the IMMULITE analyzer 1000), with the specificity of detection at 0.01 ng/mL and a coefficient of variation for inter- and intrasaio at 5.5%.
An automated enzymatic methodology was utilized to determine the lactate dosage, with five absorbance readings taken to determine the equivalent enzymatic activity of the analyses measured. The final result was the calculated average of the results. To increase the accuracy of the results, the samples were processed in duplicate.
The measurements were performed by the clinical analysis service of Santa Casa de Misericordia in Guaxupé, MG.
Statistical analysis
For statistical analysis, 5.0 statistica version software was used; p values <0.05 were considered statistically significant. The test used was the 2-way ANOVA with a post-hoc Duncan for data analysis, and the results are expressed as a mean ± SD.
Results
Comparing the initial values of variables, we observed that the average lactate threshold showed no differences between the two groups. Yet, when evaluating GH, changes were found.
Figure 1 and 2 illustrates the data relating to the pre and post sample lactate threshold of athletes who underwent exercises without vascular occlusion (Group 1) and vascular occlusion (Group 2). The mean lactate observed was 12.88 ± 0.9 pre-exercise and 14.44 ± 0.7 post-exercise for (Group 1). The lactate mean was 14.88 ± 0.7 pre exercise and 17.11 ± 1.25 post exercise for (group 2), showing no statistical difference (p>0.05). For more details Graphic 1
Figure 1: Exercise without vascular occlusion
Figure 2: Exercise with vascular occlusion
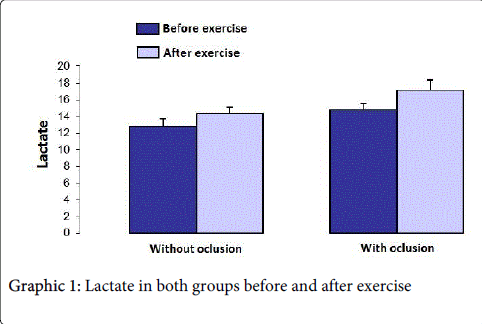
Graph 1: Lactate in both groups before and after exercise
Graphic 2 illustrates the data before and after GH in the sample of athletes who underwent exercises without vascular occlusion (Group 1) and vascular occlusion (Group 2). The GH mean was 9.53 ± 1.8 preexercise and 6.11 ± 1.5 post exercise for group 1. The GH mean was 3.63 ± 1.44 ± 6.38 pre-exercise and 2.5 post exercise for group 2, showing no statistical significance (p>0.05).

Graph 2: Growth hormone in both groups before and after exercise
When comparing the data between the groups, there were no statistically significant results (p>0.05). However, when comparing data within the groups, group 2 obtained an increase in both the lactate threshold as well as the GH; group 1, on the other hand, had an increase in the lactate threshold, and a decrease in the GH.
Discussion
This study was conducted in order to assess changes in levels of lactate and GH in male athletes submitted to muscular strengthening with or without vascular occlusion.
Based on the results, we realize that some items assessed did not present significant changes when comparing one group with another. However, as shown, there were variations in group 2 with respect to lactate and GH, which leads us to suggest that even exercise of short duration and low intensity training, when combined with vascular occlusion, can improve physical performance of young athletes through biochemical changes. Moreover, this type of activity associated with vascular occlusion had an effect equal to or superior to high intensity resistance training exercise without occlusion.
The correlation of exercise-associated vascular occlusion, lactate, and growth hormone has already been discussed in the literature. Studies show that due to a reduction in blood flow at the time of exercise, lactate accumulates in muscles. Thus, even in a lowintensity exercise, when combined with occlusion, the recruitment of additional motor units is required, and large amounts of growth hormone is released and subsequently deposited within the muscle.
However, studies show that GH has effects considered "anabolic", among which promotes positive protein balance [22], increases the amount of muscle mass dysfunction [23] and releases IGF-1 [24], which is involved in stimulating muscle hypertrophy process [23.25]. However, changes in blood lactate will not always be predictive of changes in GH, as can be observed in Chart 1. This chart illustrates pre and post exercises related to the sample lactate threshold in athletes who underwent exercise with and without vascular occlusion.
In the majority of studies, blood samples were used to determine the concentration level of GH and lactate before and after physical activities, yet few research studies present exercise results [26,27].
In a other study [28], designed to evaluate biochemical parameters, plasma levels of GH and lactate were used with 11 subjects (3 men and 8 women) with a mean age of 65 who were submitted to low resistance exercise associated with the restriction of blood flow ranging between 140-150 mmHg upon the proximal thigh. Similar to our study, blood collection was performed before the session, and 15 minutes after the session. With respect to the restriction of blood flow in this study, 100 mmHg presented an average of 1.3 times the systolic pressure for each individual [2]. In the same work performed by Yokokawa [28], there was a significant increase in GH as shown in the post hoc test (p=0.010). Of the 11 subjects studied,one male presented an increase in GH 293 times when pre-training was compared to post training (pre-exercise: 0.1 ng/ml, post-exercise: 29.3 ng/ml).
Although we found some studies concerning this research topic in the literature, we did not find a paper that compares two groups, as was the aim of our research. However, when we compared the intergroup data, there was not a significant effect (p> 0.05). But when comparing data within groups, we observed that group 2 achieved an increase in both the threshold and in lactate and GH levels. Group 1 had an increase in the lactate threshold, yet a decrease of GH.
This can be explained by the heterogeneity of the groups, which was beyond our control, since the division of the groups in question occurred randomly. In addition, variables such as level of training [29], body composition [30], gender [31] and the age of individuals studied [32] may also modulate the release of this hormone [33,34].
Sumide [35] also reported that low resistance exercise intensity associated with vascular compression may play a role in GH secretion, but some factors may influence the proper concentration, such as metabolic demand, hypoxia, and also different protocols combined with the restriction of blood flow.
In relation to a reduction in serum levels of GH in the SO group, a study [36] explains why athletes usually have lower GH release induced by exercise in sedentary or poorly trained individuals; Silva and Lengyel [37] in their studies, demonstrated that the synthesis of GH is also regulated by negative feedback. In other words, the high concentration of GH in circulation may lead to reduced stimulation of its synthesis in the adenohypophysis and/or reduced interaction with their receptors in body tissues, thus, attenuating its effects.
We believe that in order for metabolic stress to work effectively as part of high-intensity exercise endurance, there needs to be greater intensity in low-intensity resistance exercise associated with occlusion.
Although the pressure for restricting blood flow in this study was 100 mmHg, there was an average 1.3-fold by applying systolic pressure to each individual [2]. Previous studies on this topic have employed exercise intensity ranging from 20 to 50% of MR and a pressure of 50-250 mmHg [35]. Therefore, it is unclear if these training techniques are safer and more effective than standard traditional exercise.
Conclusion
This study demonstrated that the limited increase in lactate threshold and production of GH when compared to participants without occlusion (G1) and with occlusion group (G2) was not statistically significant.
However, the comparison of intra groups showed an increase in lactate threshold and a production of GH in G2, while G1 demonstrated an increase in lactate threshold, but a decrease of GH. These results suggest that the additional recruitment of GH during low-intensity exercise endurance can occur with the restriction of blood flow. This new resistance training method should be analyzed and further experiments are needed to optimize the protocol to reach an ideal level of high intensity resistance training in young athletes.
References
- Kisner C (2005) Exercíciosterapêuticos: fundamentos e técnicas. (4th edn.) Barueri, SP.
- Takarada Y, Takazawa H, Sato Y, Takebayashi S, Tanaka Y, et al. (2000) Effects of resistance exercise combined with moderate vascular occlusion on muscular function in humans.JApplPhysiol (1985) 88: 2097-2106.
- Yasuda T, Brechue WF, Fujita T, Shirakawa J, Sato Y, et al. (2009) Muscle activation during low-intensity muscle contractions with restricted blood flow.J Sports Sci 27: 479-489.
- Yasuda T, Abe T, Brechue WF (2010) Venous blood gas and metabolite response to low-intensity muscle contractions with external limb compression, Metabolism Clinical and Experimental, 59: 1510-1519.
- Ozaki H, Sakamaki M, Yasuda T, Fujita S, Ogasawara R, et al. (2011) Increases in thigh muscle volume and strength by walk training with leg blood flow reduction in older participants.JGerontol A BiolSci Med Sci 66: 257-263.
- Short KR, Moller N, Bigelow ML, Coenen-Schimke J, Nair KS (2008) Enhancement of muscle mitochondrial function by growth hormone.JClinEndocrinolMetab 93: 597-604.
- Wilmore JH, Coltill DL (2001) Fisiologia do Esporte e do Exercício. (2nd edn.) Barueri, SP, Manole.
- Loeppky JA, Gurney B, Kobayashi Y, Icenogle MV (2005) Effects of ischemic training on leg exercise endurance.JRehabil Res Dev 42: 511-522.
- Rocha RM, Bomfim DL, Nascimento RTB, Moreira SR, Simões HG (2010) A Variação do Método de Incremento de CargasNão Altera a Determinação do Limiar de LactatoemExercícioResistido. Rev. Bras. Med. Esporte 16: 282-285.
- Weltman A, Snead D, Stein P (1990) Reliability and validity of a continuous incremental treadmill protocol for the determination of lactate threshold, fixed blood lactate concentrations, and VO2max. Int J Sports Med 11: 26-32.
- Rowell LB, Shepherd JT (1996) Handbook of Physiology - Exercise: Regulation and integration of multiple systems. New York: Oxford University Press pp: 616-648.
- West DW, Kujbida GW, Moore DR (2009) Resistance exercise-induced increases in putative anabolic hormones do not enhance muscle protein synthesis or intracellular signalling in young men. J Physiol 587: 5239-5247.
- Wernbom M, Augustsson J, Raastad T (2008) Ischemic strength training: a low-load alternative to heavy resistance exercise?Scand J Med Sci Sports 18: 401-416.
- Godfrey RJ, Madgwick Z, Whyte GP (2003) The exercise-induced growth hormone response in athletes.Sports Med 33: 599-613.
- Ehrnborg C, Lange KH, Dall R, Christiansen JS, Lundberg PA, et al. (2003) The growth hormone/insulin-like growth factor-I axis hormones and bone markers in elite athletes in response to a maximum exercise test.JClinEndocrinolMetab 88: 394-401.
- Van Cauter E, Copinschi G (2000) Interrelationship between growth hormone and sleep. Growth Horm, IGF Res 10: 557-562.
- Tirapegui J, Fukushima SE, Grimaldi G (1993) [Growth, somatomedin and nutrition].Arch LatinoamNutr 43: 94-104.
- van der Lely AJ (2004) Justified and unjustified use of growth hormone.Postgrad Med J 80: 577-580.
- Tirapegui J, Mendes RR, Gomes MR, Rogero MM (2005) Crescimento muscular: Nutrição, metabolismo e suplementaçãonaatividadefísica. São Paulo: Atheneupp: 119-130.
- Gomes MR, Pires I, Castro IA, Tirapegui J (2004) Effect of moderate physical exercise on plasma and tissue levels of insulin-like growth factor-1 (IGF-1) in adult rats. Nutr Res 24: 555-564.
- Santos LTA, Vale RGS, Mello DB, Giani TS, Dantas EHM (2011) Níveis de igf-1 e força muscular emidosas com disfunçõesMúsculo-esqueléticastratadas com cinesioterapia. R da EducaçãoFísica 22: 19-26.
- Fryburg DA, Gelfand RA, Barrett EJ (1991) Growth hormone acutely stimulates forearm muscle protein synthesis in normal humans.Am J Physiol 260: E499-504.
- Machida S, Booth FW (2004) Insulin-like growth factor 1 and muscle growth: implication for satellite cell proliferation.ProcNutrSoc 63: 337-340.
- Adams GR (2000) Insulin-like growth factor in muscle growth and its potential abuse by athletes.Br J Sports Med 34: 412-413.
- Chen Y, Zajac JD, MacLean HE (2005) Androgen regulation of satellite cell function.JEndocrinol 186: 21-31.
- Wideman L, Weltman JY, Hartman ML, Veldhuis JD, Weltman A (2002) Growth hormone release during acute and chronic aerobic and resistance exercise: recent findings. Sports Med 32: 987-1004.
- Kraemer WJ, Ratamess NA (2005) Hormonal responses and adaptations to resistance exercise and training.Sports Med 35: 339-361.
- Yokokawa Y, Hongo M, Urayama H, Nishimura T, Kai I (2008) Effects of low-intensity resistance exercise with vascular occlusion on physical function in healthy elderly people, Bioscic Trends 2: 117-123.
- Diego AM, Fernandez-Pastor VJ, Alvero JR, Perez F, Ruiz M (1992) Niveles de glucosa, glucagon y hormona de crescimentoplasmáticos en sujetossedentarios y entrenados en respuesta a ejerciciomáximo. Arq Med Deporte 9 : 355-360.
- Lange KH (2004) Fat metabolism in exercise--with special reference to training and growth hormone administration.Scand J Med Sci Sports 14: 74-99.
- Wideman L, Weltman JY, Shah N, Story S, Veldhuis JD, et al. (1999) Effects of gender on exercise-induced growth hormone release.JApplPhysiol (1985) 87: 1154-1162.
- Marcell TJ, Wiswell RA, Hawkins SA, Tarpenning KM (1999) Age-related blunting of growth hormone secretion during exercise may not be solely due to increased somatostatin tone. Metabolism 48: 665-670.
- Jenkins PJ (1999) Growth hormone and exercise.ClinEndocrinol (Oxf) 50: 683-689.
- Rennie MJ (2003) Claims for the anabolic effects of growth hormone: a case of the emperor's new clothes?Br J Sports Med 37: 100-105.
- Sumide T, Sakuraba K, Sawaki K, Ohmura H, Tamura Y (2009) Effect of resistance exercise training combined with relatively low vascular occlusion.JSci Med Sport 12: 107-112.
- Cruzat VF, Junior JD, Jirapegue J, Schneider CD (2008) Hormônio do crescimento e exercíciofísico: consideraçõesatuais. Revistabrasileira de ciênciasfarmacêuticas, 44: 549-562.
- Silva SRC, Lengyel AM (2003) Influência dos glicocorticóidessobre o eixosomatotrófico. Arq. Bras. Endocrinol. Metab 47: 388-397.
Relevant Topics
- Child Health Education
- Construction Safety
- Dental Health Education
- Holistic Health Education
- Industrial Hygiene
- Nursing Health Education
- Occupational and Environmental Medicine
- Occupational Dermatitis
- Occupational Disorders
- Occupational Exposures
- Occupational Medicine
- Occupational Physical Therapy
- Occupational Rehabilitation
- Occupational Standards
- Occupational Therapist Practice
- Occupational Therapy
- Occupational Therapy Devices & Market Analysis
- Occupational Toxicology
- Oral Health Education
- Paediatric Occupational Therapy
- Perinatal Mental Health
- Pleural Mesothelioma
- Recreation Therapy
- Sensory Integration Therapy
- Workplace Safety & Stress
- Workplace Safety Culture
Recommended Journals
Article Tools
Article Usage
- Total views: 18801
- [From(publication date):
April-2015 - Aug 29, 2025] - Breakdown by view type
- HTML page views : 14112
- PDF downloads : 4689