The Problem of Sedentary Behaviour in the Office Workspace: A Structured Exercise Program for Primary Prevention
Received: 14-Mar-2018 / Accepted Date: 17-May-2018 / Published Date: 18-May-2018 DOI: 10.4172/2165-7025.1000392
Abstract
Occupations that require employees to remain seated for extended periods of time are continually becoming more pervasive in today’s workforce. Those who perform office/desk work are sitting on average 8-12 hours/day during work days, and 7-9.5 hours/day on days off. These trends are particularly worrisome considering higher prevalence for conditions such as metabolic syndrome, type 2 diabetes, obesity, deep vein thrombosis, and cardiovascular disease have been linked with habitual sedentary behaviour. The aim of this study is to briefly review pertinent research literature demonstrating the relationship between prolonged physical immobilization and the risks it has on health. Then we propose a solution in the form of a structured physical activity program. The exercises outlined in the physical activity program are supported by current research literature, do not require equipment, and can be smoothly integrated into daily routine without changing out of office attire. Implementing these exercises into daily life is designed to break up extended bouts of sitting and in turn mitigate participant’s risk of obesity, cardiovascular disease, and deep vein thrombosis. In addition to reducing these health risks individuals can also experience an increased mobility of the neck, shoulder, and scapula with continued participation.
Keywords: Office worker; Sedentary; Occupational health; Cardiovascular disease; Exercise; Physical activity
Introduction
According to the 2008 Federal Physical Activity Guidelines in the United States, only 21% of adults met the recommended guidelines for aerobic and strengthening activity [1]. Health statistics in Canada revealed similar findings in the adult population with a mere 15% meeting the weekly moderate-to-vigorous physical activity guideline [2]. This trend is particularly worrisome considering the detrimental effects prolonged immobilization has on health outcomes. Recent findings have linked habitual sedentary behaviour to higher prevalence of metabolic syndrome, type 2 diabetes, obesity, and cardiovascular disease (CVD) [3]. Additional research found positive correlations between increased sedentary time and all-cause mortality and cancer incidence [4].
Occupations that require employees to remain seated for extended periods of time are continually becoming more pervasive in today’s workforce [5,6]. Individuals with sedentary occupations are sitting for an average of 10.0 ± 2.0 hours/day during work days and 8.1 ± 1.4 hours/day on days off 7. These occupations frequently expose employees to prolonged periods with poor posture and repetitive movements of the upper extremity, both of which have been linked as causes of neck and shoulder pain [7]. Prolonged immobilization of the lower extremity has also been shown to increase the risk of conditions such as deep vein thrombosis (DVT) [8]. As a result, designing an exercise program for office workers that does not require the use of specialized equipment and can be seamlessly incorporated into their daily routine during work hours is paramount. The risk of deep vein thrombosis can be decreased when leg muscles are worked on a basis of at least every 2-3 hours [8]. In contrast, the American Diabetes Association suggests spending no longer than 30 continuous minutes in a sedentary position to reduce the risk of developing type 2 diabetes [9]. Due to this variability, it is recommended to err on the side of caution and break up sedentary behaviour with exercises or stretches at least every 2-3 hours. This interval provides a great opportunity to stand up and stretch and will be the basis in terms of frequency this exercise program should be employed. Short breaks of 1-2 minutes should also be made every 30 minutes or at the workers’ discretion.
Several wearable devices and lifestyle applications that provide feedback on sedentary time and physical activity habits have become a trending piece of technology in the fitness industry. Many of these lifestyle applications have proven useful for sending push notifications reminding individuals to stand up and stretch. In addition to push notifications, many wearable devices and lifestyle applications also possess tools allowing for social comparison. Comparing physical activity levels socially is shown to be advantageous in increasing the amount individuals walk as well as their overall level of physical activity [10]. These devices and fitness applications would likely not benefit an office worker due to the occupation typically requiring the employee to work from a desk. Due to this underlying sedentary nature of office work it is often not possible to implement the activities suggested by the device (i.e. go for a run) at their recommended intervals. This SEPro can be implemented as an effective alternative to the use of devices and fitness applications. The ideal exercise regimen for an office worker involves reducing the risk of obesity, type 2 diabetes, cardiovascular disease, and deep vein thrombosis while increasing core muscular strength, and mobility of the neck and shoulders. These factors are not adequately addressed by current wearable devices or fitness applications.
Recommendation: A Structured Exercise Program (SEPro)
Program basics
This physical activity program aims to increase mobility and reduce the risks associated with prolonged sitting in office workers by incorporating full body stretches and exercises that work on improving joint stability, reinforcing proper sitting posture mechanics, and strengthening weak muscles. Each stretch or exercise is designed to be easy to learn, non-embarrassing, carry a low risk of injury, and not require more than a few minutes to complete while at the workstation. This program is designed in a way that it can be integrated into the employee’s lifestyle while at the office. The program can be completed within 15-20 minutes depending on the number of sets and repetitions being performed for each exercise. Most of the exercises can be done while in a seated position and do not require the employee to use their personal break times to complete. All sets and repetitions are provided as guidelines as a means to yield the ideal result. It is likely the beneficial effects of each exercise remain present to a lesser degree even if the recommended numbers of sets are not being fully achieved. For safety precautions it is recommended participants breathe normally throughout all exercises to avoid a Valsalva maneuver or in other words, a forcible exhalation against a closed glottis. This practice thereby increases thoracic cavity pressure and decreases venous return to the heart [11].
Advantages of a workplace exercise program
Having an exercise program specifically designed to combat the physical demands of office work is paramount. This program has several advantages over general exercise programs and others claiming to cater to the needs of office workers. When reflecting on the practicality of the SEPro one will notice that it can be completed entirely while in business/office attire and without the use of special exercise equipment. Furthermore, it can be completed within the comfort of the employee’s own workspace, preventing drawing unwanted attention thus reducing the likelihood of embarrassment. All exercises within this package provide the benefit of breaking up prolonged periods of sedentary behaviour which have been shown by current research literature to reduce many negative health outcomes. Due to the nature of this program it is also very inexpensive to implement and participate in. Furthermore, there are potential advantages for the employer if their employee participates in routine exercise. We review the beneficial effects of exercise in the sections to follow.
Effects of exercise on obesity and immobility
Recent research found the annual cost attributable to obesity among full-time employees in the United States is $73.1 billion [12]. Further breaking down the costs it was found the annual economic loss in terms of lost productivity, absenteeism, and presenteeism were $6057 for obese males, and $6694 for their female counterpart [12]. Therefore, an effort to reduce the prevalence of obesity and sedentary behaviour may result in substantial economic savings for employers. The health benefits of exercise and its role in reducing the risk of obesity and increasing mobility are widely accepted in research [13-15].
Exercises to reduce the risk of cardiovascular disease
Cardiovascular diseases are the second leading cause of death among adult Canadian men and women [16]. In 2008, the Economic Burden of Illness in Canada (EBIC) identified cardiovascular disease to have the second highest total care costs out of any diagnostic category amounting to $12.1 billion [17]. Combating the risk of these diseases can be done in a variety of ways. Short bouts of physical activity throughout the day has been shown as an effective method for reducing this risk. Bilateral isometric leg extension at a knee angle of 90 degrees (Figure 1) has been shown to yield an immediate cardiovascular response. More specifically, this exercise has been shown to reduce resting and post-exercise systolic blood pressure [18].
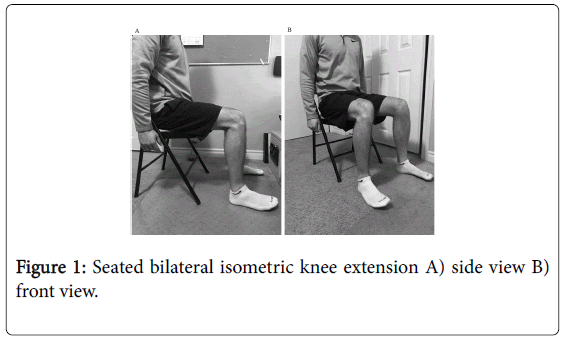
Figure 1: Seated bilateral isometric knee extension A) side view B) front view.
This exercise can be completed by sitting in a chair with your thighs roughly parallel to the ground. Once this position is achieved the individual will begin by pushing their heels into the ground by contracting the quadriceps muscle located on the front (anterior) side of their thighs. Once a contraction is felt in the anterior thigh, it is recommended the individual hold this isometric contraction for 90-120 seconds or as long as possible before relaxing. It is recommended this exercise be completed in two sets to achieve the best cardiovascular results. Depending on the individual’s current physical activity level it may be necessary to slowly progress this exercise into reaching the full amount of contraction time and number of sets.
Continuous isometric contraction during a wall squat (Figure 2) has been shown as an effective exercise for lowering resting systolic blood pressure, diastolic blood pressure, and mean arterial pressure [19].
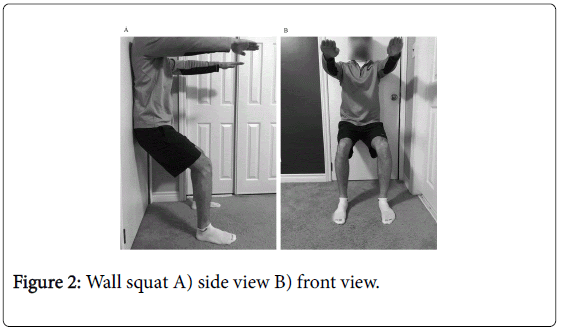
Figure 2: Wall squat A) side view B) front view.
By adjusting the angle of the knee joint, the intensity of this exercise can be increased or decreased. To start, it is recommended individuals begin performing this exercise with a slight bend at the knee and continue to progress closer towards 90 degrees as they become more comfortable. This exercise should be completed with the individuals back against a solid surface such as a wall and their feet approximately shoulder width apart. When performed correctly, this exercise should feel like the individual is sitting back into a chair. Adjusting the distance between the wall and foot placement will dictate the level in which the individual sits back. Once in the wall squat position the individual should aim for holding the position for two minutes or as long as possible to have the most beneficial effects on resting heart rate [19]. It is recommended the individual begin with completing one to two sets, and progressing until able to complete up to four sets.
Exercises to increase shoulder stability
Shoulder injuries are common when an individual is required to sit and repeatedly reach for an object. Attempting to lift or move an object that is far from the torso with a reaching movement puts unwanted stress on the stabilization muscles of the shoulder joint. These stabilization muscles, frequently called the rotator cuff, become strained or torn when the load exceeds the strength of the tissue. To increase the rotator cuffs ability to tolerate higher loads, the tissue strength itself needs to be increased.
Poor ergonomic design or lack of flexibility to change office layout typically requires office workers to sit and reach for objects on a consistent basis. In addition to rotator cuff muscles, sitting and reaching movements commonly requires activation of the serratus anterior, upper trapezius, and lower trapezius muscles. These muscles are known to oversee stabilization of the scapula. Exercises that incorporate closed kinetic chain movements are typically used in rehabilitation environments due to the beneficial effect they have on muscular strength, muscular endurance, and ability to trigger cocontractions of muscles around a joint [20]. A modified push up exercise against the edge of a desk or wall is a closed kinetic chain exercise that will strengthen the rotator cuff and dynamic stabilizers of the scapula and help reinforce a more erect posture (Figure 3). Throughout this exercise individuals should aim to maintain a neutral spine and tight core. Individuals should aim for one to two sets of 5-20 repetitions to improve muscular strength and endurance, and as a result a more stabilized shoulder [21].
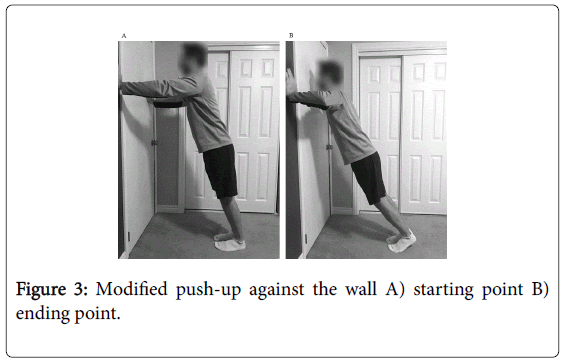
Figure 3: Modified push-up against the wall A) starting point B) ending point.
Isometric contractions of the superficial shoulder muscles are another commonly used form of exercise across current rehabilitation settings. Movements such as: shoulder adduction and abduction (Figure 4a and 4b), respectively), as well as shoulder internal and external rotation (Figure 4c and 4d) respectively) hold significant research backing as rotator cuff strengthening exercises and are commonly prescribed across many different rehabilitation settings.
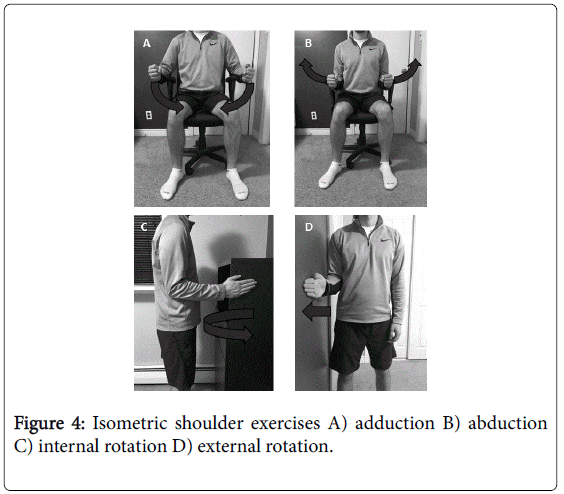
Figure 4: Isometric shoulder exercises A) adduction B) abduction C) internal rotation D) external rotation.
These exercises can be performed while seated by pressing against the armrests of a deckchair or edge of a desk to isometrically activate muscles in the shoulder. When individuals perform shoulder adduction they are pressing against the chair to pull their arms closer towards their trunk. Shoulder abduction is similar, however with this movement individuals are pushing against the armrest in a motion that would result in their arms moving farther away from their trunk. In terms of volume, research has found one to two sets of isometric contractions lasting approximately 30 seconds in length to be effective in increasing muscular strength and endurance [21,22].
Exercises reinforcing proper sitting posture
Neck pain is a prominent issue for those who do extensive computer work every day [23]. Multiple studies have associated static sitting postures with neck pain and identified poor posture mechanics and improper muscle recruitment patterns as potential contributing factors [24]. Neck strengthening exercises have been shown to reduce symptoms of neck pain and relieve tight muscles among office workers [25]. Strengthening exercises such as neck flexion (Figure 5a), neck extension (Figure 5b), and neck lateral flexion (Figure 5c and 5d) for 10-15 repetitions/direction has been shown to be most beneficial. During this exercise each repetition should be held for approximately five seconds per direction.
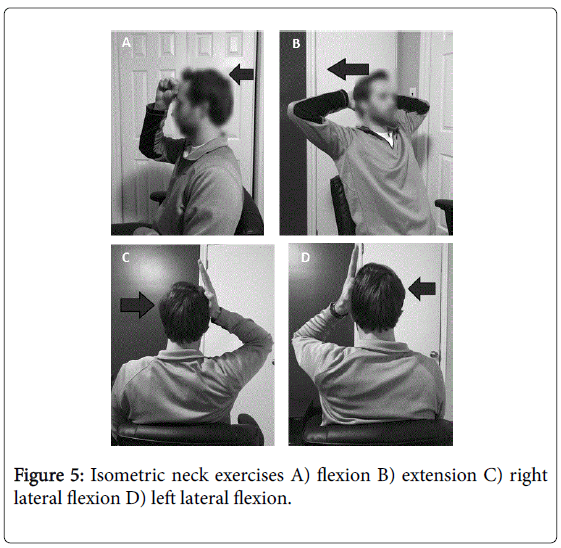
Figure 5: Isometric neck exercises A) flexion B) extension C) right lateral flexion D) left lateral flexion.
Pectoralis minor stretches combined with a scapular postural correction exercise have also been shown as effective methods for eliciting proper posture mechanics [26]. Stretching the pectoralis minor can be completed by starting with the individuals back against the wall in the stick-em up position (Figure 6). In this position the individual should attempt to keep their elbows and wrists in contact with the wall without arching their back.
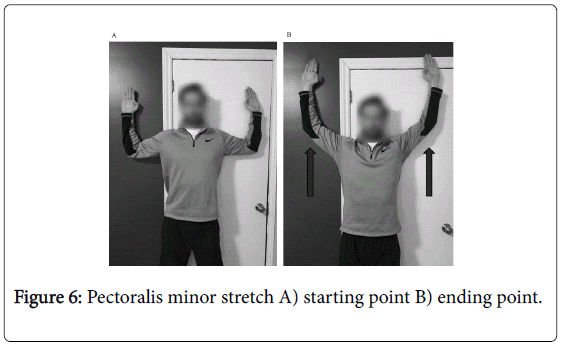
Figure 6: Pectoralis minor stretch A) starting point B) ending point.
Once the stick-em up position becomes comfortable the individual can progress the exercise by sliding their hands upwards continuing to maintain contact with their elbows and wrists against the wall (Figure 7). This stretch should be held for approximately 30 seconds and done in a total of four sets with short breaks between each set.
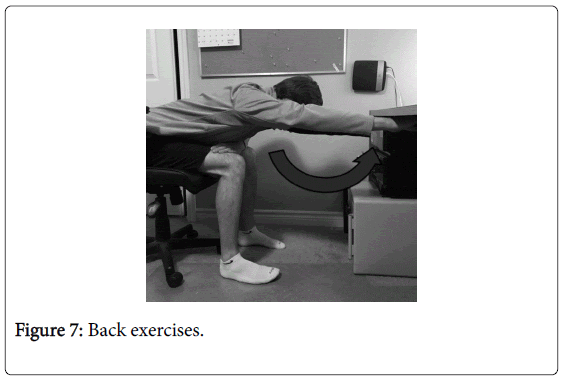
Figure 7: Back exercises.
The scapular postural correction exercise can also be completed while in a seated position. This modification should be performed without an arched back by bending forward as far as comfortably possible or until the individual’s back is approximately parallel with the ground. While remaining in this position the individual performs shoulder flexion to 180 degrees or as far as comfortably possible (reaching above their head) and holds this position for approximately five seconds (Figure 8). This exercise should be performed in up to four sets with short breaks of between 10-30 seconds between sets.
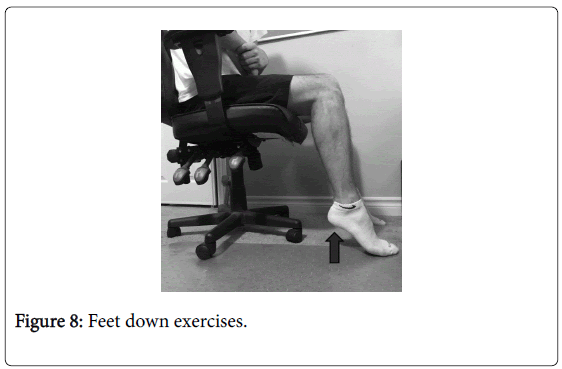
Figure 8: Feet down exercises.
Exercises to reduce the risk of deep vein thrombosis
The Centers for Disease Control and Prevention identifies physical immobilization as one of the main modifiable risk factors associated with deep vein thrombosis [8]. Research has found working from a seated position for long periods of time can increase an individual’s risk of deep vein thrombosis 3-fold [27]. Calf and toe raising exercises, while in a seated position have been commonly prescribed to reduce the risk of deep vein thrombosis [8]. Calf raises can be completed by the individual raising and lowering their heels off the ground all while keeping their toes planted on the floor (Figure 9). In contrast, toe raises should be completed by the individual raising and lowering their toes while maintaining contact on the ground with their heels (Figure 10). These two exercises may be modified by the individual pointing their toes slightly inwards, or outwards. In terms of volume, both exercises should be completed in one to two sets of 5-20 repetitions.
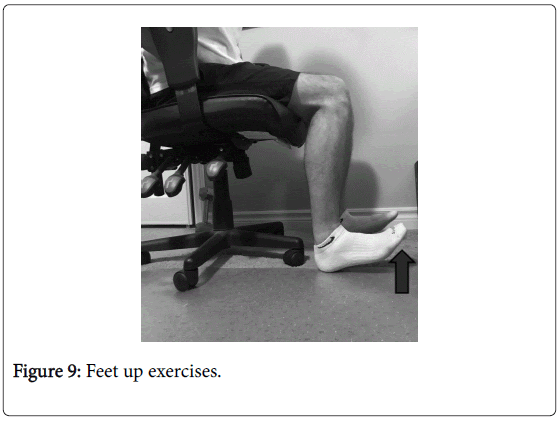
Figure 9: Feet up exercises.
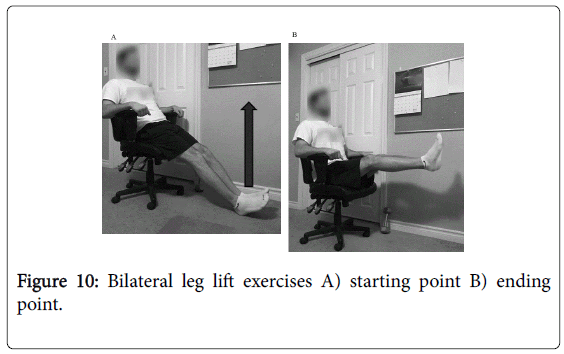
Figure 10: Bilateral leg lift exercises A) starting point B) ending point.
Core strengthening exercise
Strong core musculature is an important component in maintaining an individual’s overall musculoskeletal health. Many motions from rotational movements to bending and reaching originate from the core. Developing a strong foundation of core musculature is important to create efficient movements and reduce the likelihood of injury resulting from unnecessary load on other joints. Significant evidence has been found on the activation of abdominal muscles during bilateral leg lifts [28]. This evidence suggests individuals can strengthen core musculature by performing bilateral leg lifting exercises. To achieve maximum core activation, research suggests maintaining a neutral pelvis and keeping knees locked in full extension throughout the motion [28]. Maintaining this position throughout the full range will increase the amount of abdominal activation while reducing the amount of contribution from hip flexor musculature. By slightly leaning back into the chair individuals can allow their legs to drop more comfortably to the point where they nearly meet the floor between repetitions. This exercise should be completed in one to two sets of 5-20 repetitions.
Integrating the SEPro into Office Culture
An organization’s culture is often defined as its set of socially constructed assumptions, meanings, norms, values, and behaviour patterns [29]. Incorporating physical activity into an organization's culture can be a difficult process due to longstanding traditions, tight deadlines, unstable job security, or an overly conservative office environment. In contrast to this practice, many studies have illustrated the wide range of benefits it can have in terms of the organization and its employees [30,31]. Researchers have found office workers who take frequent breaks to engage in general exercise are less susceptible to stress, have a lower chance of developing acute and chronic muscular disorders, and have more energy throughout the day [7,32].
Sweat production while in the office may be another factor contributing to the poor integration of physical activity into mainstream office culture across North America. Many solutions such as interval exercise, maintaining a cooler environment, or exercise at an intensity of 40 watts or less (i.e. light cycling) all help reduce the amount of sweat production that might prevent someone from engaging in exercise at the workplace [33]. Aside from office workers, the employer is perhaps the second major contributor to how office culture is created. Pressure to complete tasks, extended contract positions without promise of long term employment, and mandatory overtime hours collectively contribute to an ingrained sense of urgency in employees to devote long hours to the workplace. As a result, many employees focus more heavily on the demands of their job than their personal health. Analyzing data from the 2005-2008 National Health and Nutrition Examination Survey (NHANES), the CDC found at least one third of American residents do not get enough sleep on a consistent basis. This disrupts their ability to perform daily tasks and has an accumulating effect on mental and physical health [34]. When sufficient sleep is not possible, studies have shown small breaks at work can have positive implications on productivity. Recent evidence has found short, frequent rest breaks lasting from 30 seconds to 3 minutes at 15-minute intervals improved worker productivity and well-being [35]. Short rest breaks that included small bouts of physical activity were found to be even more effective than passive rest breaks [35].
Discussion
Although the benefits of physical activity are well backed by research findings, in Canada, just 15% of adults met the weekly moderate-to-vigorous physical activity guideline. This could be explained either by shortage of time left after long periods of work, or lack of availability of special exercise equipment at the workplace. Canadian figures show office workers sit between 8-12 hours/day 7. Furthermore, recent research has shown a significant shift towards more sedentary occupations [5,6]. These worrisome findings correlate to negative consequences of inactivity and immobilization namely; obesity, type 2 diabetes, cardiovascular problems, and deep vein thrombosis [3,4,8]. Building on the previous body of literature we recognize the lack of exercise knowledge experienced by office workers resulting in habitual sedentary behaviour, and provides a practical solution for persons to participate in higher levels of physical activity [4,36,37]. The feasibility of incorporating our program in the daily routine of office workers makes it a step forward in combating the epidemic prevalence of obesity and metabolic type 2 syndrome, CVD, and musculoskeletal deconditioning.
The purpose of this program is to be implemented as a primary prevention tool to reduce the negative health risks associated with daily prolonged immobilization. This exercise program is not recommended to function as a replacement or substitution for attending a fitness facility or performing aerobic exercise. Rather, it is constructed to bridge the gap between the need of maintaining a minimum level of physical activity from one side, and the shortage of time and lack of availability of special equipment in the workplace. Furthermore, this exercise program is recommended replace the amount of daily sedentary time with light-to-moderate physical activity. Currently, office and administrative staff typically expend approximately 1.5 METs on average [38].
It is also important to distinguish this exercise program from other programs that aim to improve or maintain cardiovascular health. Due to the absence of an aerobic exercise component, this program is limited in terms of its benefits to cardiovascular health. SEPro is also not a substitute for any therapeutic exercise program that is prescribed to address a pathological musculoskeletal disease or to improve cardiac or respiratory capacity. The Canadian Society for Exercise Physiology recommends, adults aged 18-64 years accumulate at least 150 minutes of moderate-to-vigorous physical activity per week to maximize its benefit on health [39]. For adults, moderate-intensity physical activity is typically defined on an absolute scale as: 3.0-5.9 times the intensity of rest (i.e. 3.0-5.9 METs). Three exercises in this exercise program fall into the category of moderate-intensity physical activity, these being: isometric wall squats, modified push-ups, and bilateral leg lifts. Although there is no research directly measuring the MET demands of these exercises there are a few deductions that can be made. For example, researchers have found that standing at work and performing squats against resistance require approximately 3 and 5 METs respectively [38,40]. Therefore, it can be speculated that isometric wall squats, such as the type outlined in this program, likely require somewhere between 3-5 METs. The same level of deduction can be applied to the following two exercises. For example, push-ups using a moderate effort would be similar movements such as pushing a cart which require 3.8 and 4 METs respectively [40]. Therefore, an exercise such as the modified push-up likely uses in the range of 3.5-4 METs. Finally, when estimating the amount of energy expenditure for a bilateral leg lift exercise the following process can be applied. Similar activities were found, such as sit ups using a moderate effort and a general home exercise program, both of which require around 3.8 METs [40]. Therefore, due to the challenging nature of the bilateral leg lift exercise they would likely use at least 3.8 METs. Aside from these three exercises, the remainder of the SEPro can likely be classified as light-intensity physical activity. For adults, light-intensity physical activity is: 1.5-3.0 times the intensity of rest (i.e. 1.5-3.0 METs). Common examples light-intensity exercise are typically movements that do not result in sweat production, such as: mild stretching, slow walking, and light household tasks (i.e. groceries, washing dishes or cooking) [41]. Based on these guidelines, participants who only perform the moderate-intensity exercises set out in this program will still be completing at least 12 minutes/day or 84 minutes/week of moderate-intensity exercise. According to Canadian guidelines, this results in 56% of the ideal weekly moderate-intensity physical activity [39]. It is important to note this assumption is based on the participant completing the full recommended sets and repetitions for each moderate-intensity exercise. Viewing this program more holistically, this does not consider the remaining exercises classified as lightintensity physical activity. Currently, Canadian government guidelines do not provide a recommended daily volume for light-intensity physical activity, in spite of its favorable association with health [42,43]. Therefore, at this time it can be said that continuing to incorporate these light-intensity exercises will only further enhance the health benefits of participating in this program.
Predicting direct results of this exercise program on health risk factors is a challenging endeavor. Periodic, low intensity exercise performed at short intervals has been shown to lower the risk of diabetes and DVT without the undesirable production of sweat8. Moreover, repeated neck strengthening exercises would reduce the probability of neck and upper body aches [25]. Additionally, isometric exercises for shoulder muscles enhance the stability of the shoulder joint and decrease the likelihood of developing rotator cuff tendinopathy. To augment exercise adherence, we encourage the utilization of modern technology in terms of: wearable devices and lifestyle applications that provide feedback on sedentary time or push reminders to exercise.
To ensure safe outcome it is essential to consider contraindications or precautions for increasing the METs or heart and/or respiratory rate. Therefore, individuals should consult their family physician concerning heart and lungs problems prior to participating in the SEPro. In addition, a health care provider should be consulted if an individual has been experiencing a longstanding undiagnosed issue or underlying musculoskeletal disease, including but not limited to: shoulder, knee, hip, neck, back, etc.
Limitations
This exercise program is not without limitations. As a result, careful consideration should be exercised when interpreting and implementing the contents of this package. This exercise program is intended and designed for the general office worker. Special considerations and individual differences were not taken into account when designing each exercise, therefore hindering the individualization of the program. While reviewing scientific literature the search was confined to English-only publications. This limitation may have led to a language or cultural bias during the review process. We believe that this had a minimal effect upon the recommended exercises or suggestions for their implementation. The search process implemented primarily focused on articles mentioning sedentary adult populations. A third limitation is the inability to quantify the magnitude each health risk is mitigated by as a direct result of exercise. At this time the extent in which each condition is reduced likely depends on many different individual factors. Exercise adherence and technique, family history and genetics, previous health history, and total amount of leisure sedentary time are a few of the main contributing risk factors. Future research is required to quantify the reduction in risk for each health condition mentioned as a direct result of this exercise program. Therefore, at this time, the magnitude to which each risk is expected to lower as a result of this exercise program is still uncertain. It is important to note the strong body of research literature that does exist showing harmful associations of prolonged sedentary behaviour becoming less pronounced as exercise increases 4.
Conclusion
Most office workers are sedentary and confined to their workspace, often in a seated position. Over time this behaviour can lead to increased health risks including metabolic syndrome, type 2 diabetes, obesity, deep vein thrombosis, and cardiovascular disease. Therefore, breaking up these periods of prolonged immobilization with periodic short bouts of physical activity is paramount. The exercise program proposed in this study is based on pertinent research literature and provided as an introduction and stepping stone towards a more physically active lifestyle. It is important to keep in mind this program is designed to be implemented as a means of breaking up extended periods of sitting and not as a replacement or substitution for current aerobic or resistance-based exercise programs. Participants engaging in this SEPro can experience a reduced risk of obesity, cardiovascular disease, and deep vein thrombosis. In addition to increased core muscular strength, other potential benefits of this exercise program are an increased mobility of the neck, shoulder, and scapula. Further research is necessary to determine the potential benefits of this exercise program, however, there is a robust existing literature that suggests the benefits of physical activity therefore we recommend implementing it.
Funding
The authors report that there was no funding source for the work that resulted in the article or the preparation of the article.
Disclosure (Authors)
The authors declare no conflicts of interest.
References
- Blackwell DL, Lucas JW, Clarke TC (2014) Summary health statistics for U.S. adults: National health interview survey, 2012. Vital Health Stat 10: 1-161.
- Colley RC, Garriguet D, Janssen I, Craig CL, Clarke J, et al. (2011) Physical activity of canadian children and youth: Accelerometer results from the 2007 to 2009 canadian health measures survey. Heal Reports 15-23.
- Hamilton MT, Hamilton DG, Zderic TW (2007) Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 56: 2655-2667.
- Biswas A, Oh PI, Faulkner GE, Bajaj RR, Silver MA, et al. (2015) Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults a systematic review and meta-analysis. Ann Intern Med 162: 123-132.
- Kirk MA, Rhodes RE (2011) Occupation correlates of adults’ participation in leisure-time physical activity: A systematic review. Am J Prev Med 40: 476-485.
- Straker L, Mathiassen SE (2009) Increased physical work loads in modern work - A necessity for better health and performance? Ergonomics 52: 1215-1225.
- McCrady SK, Levine JA (2009) Sedentariness at work: How much do we really sit. Obesity 17: 2103-2105.
- Division of Blood Disorders National Center on Birth Defects and Developmental Disabilities C for DC and P. Venous Thromboembolism (Blood Clots). U.S. Department of Health & Human Services.
- Association AD. What Can Physical Activity Do for Me? American Diabetes Association.
- Lyons EJ, Lewis ZH MB (2014) Behavior Change Techniques Implemented in Electronic Lifestyle Activity Monitors: A Systematic Content Analysis. J Med Internet Res 16: e192.
- Gorlin R, Knowles JH, Storey CF (1957) The valsalva maneuver as a test of cardiac function. Am J Med 22:197-212.
- Finkelstein EA, DiBonaventura MDC, Burgess SM, Hale BC (2010) The costs of obesity in the workplace. J Occup Environ Med 52: 971-976.
- Bray GA, Frühbeck G, Ryan DH, Wilding JPH (2016) Management of obesity. Lancet 387: 1947-1956.
- Guilbert JJ (2003) The world health report 2002 - reducing risks, promoting healthy life. Educ Health (Abingdon) 16: 230.
- Services USDOHAH (1996) Physical Activity and Health: A Report of the Surgen General. Rev Prat 60: 1996.
- Public Health Agency of Canada. About heart diseases and conditions. Government of Canada.
- Public Health Agency of Canada. Economic Burden of Illness in Canada (2014).
- Devereux GR, Wiles JD, Howden R (2014) Immediate post-isometric exercise cardiovascular responses are associated with training-induced resting systolic blood pressure reductions. Eur J Appl Physiol 115: 327-333.
- Wiles JD, Goldring N, Coleman D (2017) Home-based isometric exercise training induced reductions resting blood pressure. Eur J Appl Physiol 117: 83-93.
- Wang CH, McClure P, Pratt NE, Nobilini R (1999) Stretching and strengthening exercises: Their effect on three- dimensional scapular kinematics. Arch Phys Med Rehabil 80: 923-929.
- Ratte-Larouche M, Szekeres M, Sadi J, Faber KJ (2017) Rotator cuff tendon surgery and postoperative therapy. J Hand Ther 30: 147-157.
- Myers NL, Toonstra JL, Smith JS, Padgett CA, Uhl TL (2015) Sustained Isometric Shoulder Contraction on Muscular Strength and Endurance: a Randomized Clinical Trial. Int J Sports Phys Ther 10: 1015-1025.
- Cagnie B, Danneels L, Van Tiggelen D, De Loose V, Cambier D (2007) Individual and work related risk factors for neck pain among office workers: A cross sectional study. Eur Spine J 16: 679-686.
- Szeto GPY, Straker L, Raine S (2002) A field comparison of neck and shoulder postures in symptomatic and asymptomatic office workers. Appl Ergon 33: 75-84.
- Andersen LL, Christensen KB, Holtermann A, Poulsen OM, Sjøgaard G, et al. (2010) Effect of physical exercise interventions on musculoskeletal pain in all body regions among office workers: A one-year randomized controlled trial. Man Ther 15: 100-104.
- Lee J hyun, Cynn H seock, Yoon T lim, Ko CH, Choi WJ, et al. (2015) The effect of scapular posterior tilt exercise, pectoralis minor stretching, and shoulder brace on scapular alignment and muscles activity in subjects with round-shoulder posture. J Electromyogr Kinesiol 25: 107-114.
- Eekhoff EM1, Rosendaal FR, Vandenbroucke JP (2003) Minor events and the risk of deep venous thrombosis. Thromb Haemost 83: 408-411.
- Andersson EA, Nilsson J, Ma Z, Thorstensson A (1997) Abdominal and hip flexor muscle activation during various training exercises. Eur J Appl Physiol Occup Physiol 75: 115-123.
- Carr LJ, Walaska KA, Marcus BH (2012) Feasibility of a portable pedal exercise machine for reducing sedentary time in the workplace. Br J Sports Med 46: 430-435.
- Lara A, Yancey AK, Tapia-Conye R, Flores Y, Kuri-Morales P, et al. (2008) Pausa para tu Salud: reduction of weight and waistlines by integrating exercise breaks into workplace organizational routine. Prev Chronic Dis 5: A12.
- Søgaard K, Blangsted AK, Nielsen PK, Hansen l, Andersen LL, et al. (2012) Changed activation, oxygenation, and pain response of chronically painful muscles to repetitive work after training interventions: A randomized controlled trial. Eur J Appl Physiol 112: 173-181.
- Koren K, Pišot R, Šimunic B (2016) Active workstation allows office workers to work efficiently while sitting and exercising moderately. Appl Ergon 54: 83-89.
- Report MW (2011) Unhealthy sleep-related behaviors--12 States, 2009. MMWR Morb Mortal Wkly Rep 60: 233-238.
- Henning RA, Jacques P, Kissel GV, Sullivan AB, Alteras-Webb SM (1997) Frequent short rest breaks from computer work: Effects on productivity and well-being at two field sites. Ergonomics 40: 78-91.
- Schmid D, Leitzmann MF (2014) Television viewing and time spent sedentary in relation to cancer risk: A meta-analysis. J Natl Cancer Inst 106: 1-19.
- Wilmot EG, Edwardson CL, Achana FA, Davies MJ, Gorely T, et al. (2012) Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 55: 2895-2905.
- Ainsworth BE, Haskell WL, Leon AS, Jacobs DR Jr, Montoye HJ, et al. (1993) Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc 25: 71-80.
- Csep (2011) Effects of Exercise Training on Plasma Lipids and Lipoproteins. Applied Physiology.
- Ainsworth BE, Haskell WL, Herrmann SD, Meckes N, Bassett DR Jr, et al. (2011) Compendium of physical activities: A second update of codes and MET values. Med Sci Sports Exerc 43: 1575-1581.
- Ainsworth BE, Haskell WL, Whitt MC, Irwin ML, Swartz AM, et al. (2000) Compendium of Physical Activities: an update of activity codes and MET intensities. Med Sci Sport Exerc 32: S498-S516.
- Buman MP, Hekler EB, Haskell WL, Pruitt L, Conway TL, et al. (2010) Objective light-intensity physical activity associations with rated health in older adults. Am J Epidemiol 172: 1155-1165.
- Loprinzi PD, Lee H, Cardinal BJ (2015) Evidence to support including lifestyle light-intensity recommendations in physical activity guidelines for older adults. Am J Heal Promot 29: 277-284.
Citation: Mann S, Hamad AH, Kumbhare D (2018) The Problem of Sedentary Behaviour in the Office Workspace: A Structured Exercise Program for Primary Prevention. J Nov Physiother 8: 392. DOI: 10.4172/2165-7025.1000392
Copyright: © 2018 Mann S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Select your language of interest to view the total content in your interested language
Share This Article
Recommended Journals
Open Access Journals
Article Tools
Article Usage
- Total views: 12897
- [From(publication date): 0-2018 - Dec 13, 2025]
- Breakdown by view type
- HTML page views: 11684
- PDF downloads: 1213