 Spanish
Spanish  Chinese
Chinese  Russian
Russian  German
German  French
French  Japanese
Japanese  Portuguese
Portuguese  Hindi
Hindi Our Group organises 3000+ Global Conferenceseries Events every year across USA, Europe & Asia with support from 1000 more scientific Societies and Publishes 700+ Open Access Journals which contains over 50000 eminent personalities, reputed scientists as editorial board members.
Open Access Journals gaining more Readers and Citations
700 Journals and 15,000,000 Readers Each Journal is getting 25,000+ Readers
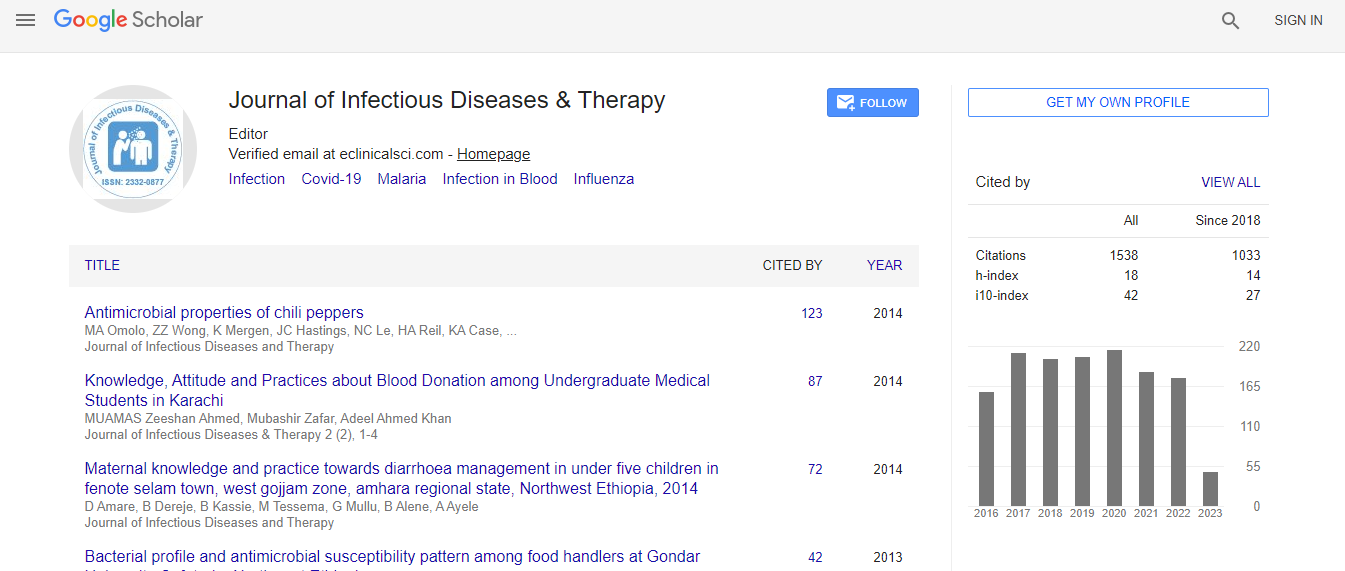
Google Scholar citation report
Citations : 1529
Journal of Infectious Diseases & Therapy received 1529 citations as per Google Scholar report
Indexed In
- Index Copernicus
- Google Scholar
- Open J Gate
- RefSeek
- Hamdard University
- EBSCO A-Z
- OCLC- WorldCat
- Publons
- Euro Pub
- ICMJE
Useful Links
Recommended Journals
Related Subjects
Share This Page
Osteoporosis: Update and emerging therapies
Global Experts Meeting on Infectious Diseases, Diabetes and Endocrinology
Mohammad Saifuddin
Dhaka Medical College and Hospital, Bangladesh
Posters & Accepted Abstracts: J Infect Dis Ther
Abstract
Osteoporosis is a growing major public health prob¬lem with impacts on quality and quantity of life that cross medical, social and economic lines. National Osteoporosis Foundation (NOF) estimates that 10.2 million Americans have osteoporosis and that an additional 43.4 million have low bone mass. More than 2 million osteoporosis-related fractures occur annually in the U.S.A. and more than 70% of these occur in women. Despite the availability of cost effective and well-tolerated treatments to reduce fracture risk, only 23% of women age 67 or older who have an osteoporosis-related fracture receive either a bone mineral density test or a prescription for a drug to treat osteoporosis in the six months after the fracture. Lifelong adequate calcium and vitamin D intake is necessary for the acquisition of peak bone mass and subsequent maintenance of bone health. Current FDA-approved pharmacologic options for the prevention and/or treatment of postmenopausal osteoporosis include, in alphabetical order: Bisphosphonates (alendronate, alendronate plus D, ibandronate, risedronate and zoledronic acid), calcitonin, estrogens (estrogen and/or hormone therapy), estrogen agonist/antagonist (raloxifene), tissue-selective estrogen complex (conjugated estrogens/bazedoxifene), parathyroid hormone (PTH[1-34], teriparatide) and the RANKL inhibitor denosumab. Sequential treatment with anabolic therapy followed by an anti-resorptive agent is generally preferred. Combination therapy with teriparatide and an anti-resorptive can be considered in a few clinical settings in patients with very severe osteoporosis such as spine and hip fractures. There are few indications for combining two anti-resorptive treatments, but such options could be considered in the short-term in women who are experiencing active bone loss while on low dose HRT for menopausal symptoms or raloxifene for breast cancer prevention. Evidence of efficacy beyond five years is limited, whereas rare safety concerns such as ONJ and atypical femur fractures become more common beyond five years. Since there is no extensive evidence base to guide treatment duration decisions, duration decisions need to be individualized. After the initial three to five-year treatment period, a comprehensive risk assessment should be performed. This should include interval clinical history, particular with respect to intercurrent fracture history and new chronic diseases or medications, as well as height measurement, BMD testing and vertebral imaging if there has been any documented height loss during the treatment period. It is reasonable to discontinue bisphosphonates after three to five years in people who appear to be at modest risk of fracture after the initial treatment period. In contrast, for those who appear to be at high risk for fracture, continued treatment with a bisphosphonate or an alternative therapy should be considered.Biography
E-mail: saifk56dmc@yahoo.com