 Spanish
Spanish  Chinese
Chinese  Russian
Russian  German
German  French
French  Japanese
Japanese  Portuguese
Portuguese  Hindi
Hindi Our Group organises 3000+ Global Conferenceseries Events every year across USA, Europe & Asia with support from 1000 more scientific Societies and Publishes 700+ Open Access Journals which contains over 50000 eminent personalities, reputed scientists as editorial board members.
Open Access Journals gaining more Readers and Citations
700 Journals and 15,000,000 Readers Each Journal is getting 25,000+ Readers
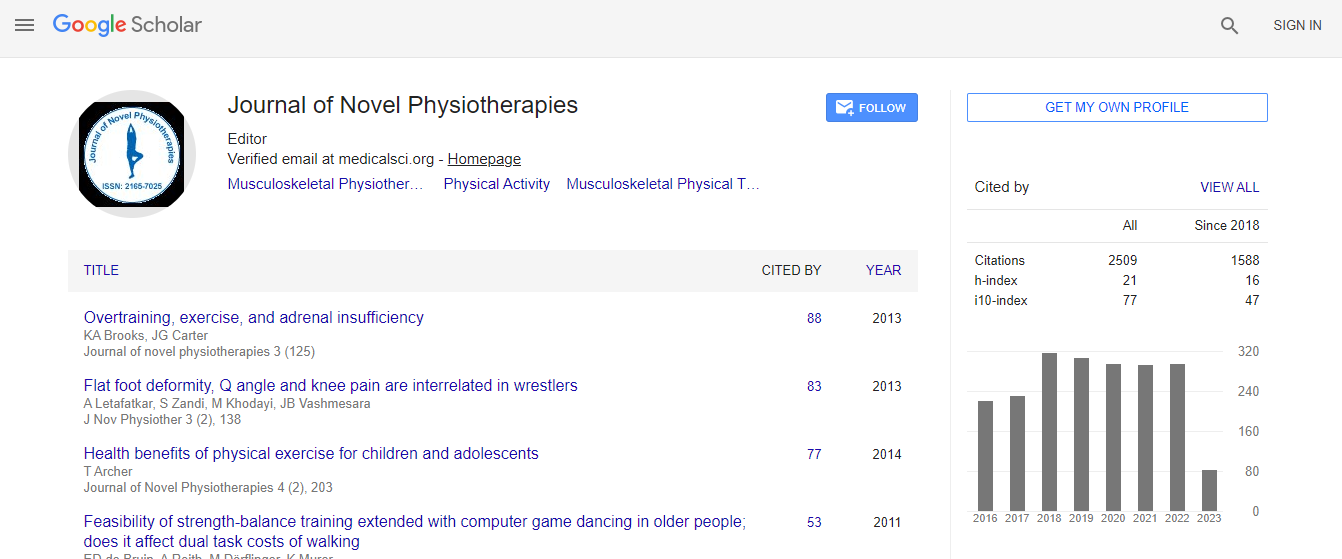
Google Scholar citation report
Citations : 3145
Journal of Novel Physiotherapies received 3145 citations as per Google Scholar report
Journal of Novel Physiotherapies peer review process verified at publons

Indexed In
- Index Copernicus
- Google Scholar
- Open J Gate
- Genamics JournalSeek
- Academic Keys
- SafetyLit
- RefSeek
- Hamdard University
- EBSCO A-Z
- OCLC- WorldCat
- Publons
- ICMJE
Useful Links
Recommended Journals
Related Subjects
Share This Page
Rehabilitative approach of pelvic floor dysfunctions
2nd International Conference and Expo on Novel Physiotherapies
Naglaa A Gadallah
Ain Shams University, Egypt
Posters & Accepted Abstracts: J Nov Physiother
Abstract
The common denominator in pelvic floor dysfunctions is now recognized as being neuro-muscular. Neurophysiology is assuming an ever increasing role in the diagnosis and management of pelvic floor disorders which may be caused by nerve dysfunction, non-relaxing pelvic floor muscles or both. Urologic disorders and pelvic pain present an obvious relationship. The majority of the urologic chronic pelvic pain syndromes arise from either a possible urinary bladder source known as interstitial cystitis or prostate source known as prostate pain syndrome. Patients��? evaluation should start with detailed history and examination. Neurophysiological studies as urodynamics, manometry studies and electrodiagnosis (as EMG, pudendal nerve conduction studies, sacral reflexes and evoked potentials) are helpful in assessing dysfunctions. Rehabilitation of pelvic floor dysfunctions is individualized, depending on the specific etiology. Conservative therapies include behavior modification, pelvic floor therapy, and biofeedback therapy, percutaneous stimulation of the posterior tibial nerve and myofascial release techniques of trigger points. Botulinum toxin injection is effective in reducing urethral sphincter resistance or detrusor overactivity and is used also in treating chronic obstructive constipation. Sacral neuromodulation can be used in the management of refractory voiding dysfunction or selected cases of fecal incontinence.Biography
Email: naglagadallah1@hotmail.com