 Spanish
Spanish  Chinese
Chinese  Russian
Russian  German
German  French
French  Japanese
Japanese  Portuguese
Portuguese  Hindi
Hindi Our Group organises 3000+ Global Conferenceseries Events every year across USA, Europe & Asia with support from 1000 more scientific Societies and Publishes 700+ Open Access Journals which contains over 50000 eminent personalities, reputed scientists as editorial board members.
Open Access Journals gaining more Readers and Citations
700 Journals and 15,000,000 Readers Each Journal is getting 25,000+ Readers
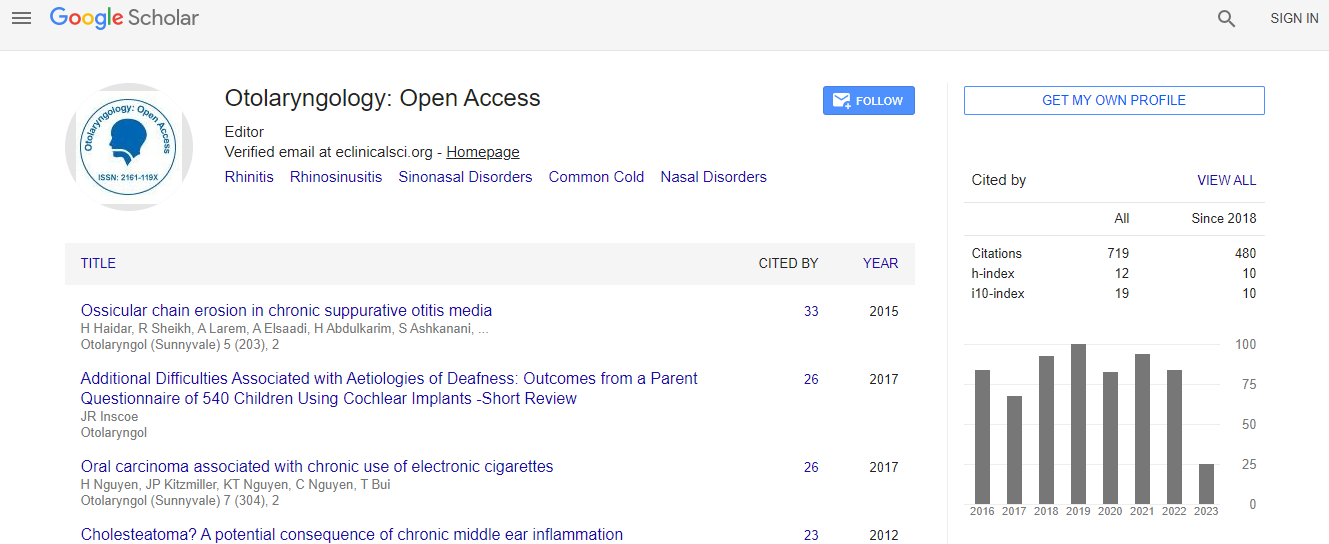
Google Scholar citation report
Citations : 925
Otolaryngology: Open Access received 925 citations as per Google Scholar report
Otolaryngology: Open Access peer review process verified at publons

Indexed In
- Index Copernicus
- Google Scholar
- Sherpa Romeo
- Open J Gate
- Genamics JournalSeek
- RefSeek
- Hamdard University
- EBSCO A-Z
- OCLC- WorldCat
- Publons
- Geneva Foundation for Medical Education and Research
- ICMJE
Useful Links
Recommended Journals
Related Subjects
Share This Page
The skull vibration induced nystagmus test (SVINT): Clinical benefit in unilateral vestibular lesions and anterior canal dehiscence diagnosis
5th Global Summit and Expo on Head, Neck and Plastic Surgery
G Dumas
Clinique ORL CHU Grenoble, France
ScientificTracks Abstracts: Otolaryngol (Sunnyvale)
Abstract
Background & Aim: Vibrations applied to skull produce a vibration induced nystagmus (VIN) in unilateral vestibular lesions (UVL). These responses described for the first time by L�?¼cke in 1976 were confirmed and extended by Hamann, et al. and our group in Grenoble in 1999. A VIN induced by cervical vibrations has also been described but involves different somatosensory inputs and centers. Moreover, bone conducted vibrations stimulate utricle (oVEMP) or sacculus (cVEMP) and muscular cervical stimulations influence posture. Our purpose was to clarify this initial design, the actual inner ear target of this test restricted to bone conduction stimulation (which we term the Skull Vibration Induced Nystagmus Test (SVINT)), to find out optimal stimulation locations and frequencies, to show possible clinical interest of the VIN primarily in unilateral lesions (UVL) and superior canal dehiscence (SCD). In animals, Curthoys demonstrated at 100 Hz a stimulation of both canalar and otolithic structures (type I inner ear cells) and at 500 Hz a specific stimulation of otolithic irregular fibers. Material & Methods: 19500 patients with total or partial peripheral unilateral lesions (TUVL/PUVL) or superior semicircular canal dehiscence (SCD) were studied with the Synapsys 3F vibrator (30, 60, 100 Hz) and the (10-800 Hz) Bruel & Kjaer Vibrator applied on vertex and each mastoids and recorded under VNG 2D or 3D. The results were compared with those in 95 normal subjects and 34 brainstem lesions. Results: The test is positive when it generates a VIN beating toward the same direction whatever the skull location, sustained, repeatable, starting with the stimulation and stopping with it. Optimal frequency is 100 Hz in patients with normally encased labyrinth; the best location is the mastoid in UVL except in SCD (higher responses are obtained on vertex). Both labyrinths are concomitantly stimulated and VIN is the result of the stimulation of the intact side in TUVL. In PUVL, a VIN beating toward the intact side is usually obtained but in SCD, VIN beats toward the lesion side (bone conduction facilitation) and is observed at higher frequencies. The VIN slow phase velocity (SPV) is correlated in TUVL with the total caloric efficiency on the healthy ear. No responses are observed in bilateral symmetrical lesions. VIN is permanent in TUVL. Sensitivity is 98% in TUVL and specificity 94% in normal subjects. In PUVL, sensitivity is 75% and VIN beats toward the intact side in 91% of cases. No significant alteration of the vestibulo-spinal reflex analyzed with posturography was observed in chronic compensated UVL. SVINT is more sensitive to reveal peripheral than central diseases. Conclusion: SVINT is a global vestibular test at 100 Hz and acts as a vestibular Weber test. It explores the vestibulo-ocular reflex and complements the CaT, the HST and the HIT in the vestibule multi-frequency analysis. In clinical practice, it can substitute the water caloric test in case of middle or external ear pathologies. SVINT is useful to detect instantaneously as a bedside first line examination test, a vestibular asymmetry. It usually reveals a lesional nystagmus in common UVL peripheral patients and an excitatory VIN in SCD. It is more sensitive to reveal peripheral than central diseases. The VIN is not modified by the vestibular compensation mechanisms and involves type I inner ear sensory cells.Biography
G Dumas is a consultant at Clinique ORL CHU GRENOBLE, France. He completed his doctorate in medicine in 1980 on a topic “Kanamycin transplacentar ototoxic effect in rats”. He is also an active member of multiple Scientific Societies such as Fellow of the French ENT and cervico-facial pathology society (S.F.ORL); the Audiology French society; the international otoneurology society (SIO); the international vestibular rehabilitation society (SIRV). He is a Member of the Laboratory Development, Adaptation and Disadvantage (EA 3450 DevAH) – University of Lorraine.
Email: GDumas@chu-grenoble.fr